

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Tako-Tsubo cardiomyopathy (TTC) is a reversible cardiomyopathy mimicking acute myocardial infarction. It most commonly affects postmenopausal women and is characterized by a transient left ventricular (LV) apical ballooning without epicardial coronary artery disease.1) It is clinically characterized by acute chest pain or dyspnea in most cases and transient ST elevation in the acute phase. Troponin level is often slightly elevated.
The prognosis is generally good.2) Severe emotional stress is the most common trigger for this syndrome in the published cases, but it can also be precipitated by other possible etiologies. We present a case of a patient with TTC triggered by misdirection while swallowing the drug pills.
Case
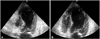
We report the case of a 67-year-old woman with hypertension and no history of coronary disease hospitalized in the Gastro-Intestinal department for treatment of severe malnutrition. Her past medical history was significant for a total gastrectomy for gastric neoplasia 5 years ago with complete remission. She was being supplemented by enteral feeding via a nasogastric tube. She had no history of recent emotional stress. While swallowing the drug pills during hospitalization, she suffered overnight from a misdirection (false route), but due to a hacking cough an inhalation pneumonia was avoided and later she complained of constrictive chest pain. The per-critical electrocardiography (ECG) showed sinus rhythm with an anterior ST-segment elevation (Fig. 1). A diagnosis of an acute myocardial infarction was made and she was taken to the cardiac catheterization laboratory for primary percutaneous coronary intervention. The coronary angiography demonstrated a non-obstructive coronary atheroma. The LV angiography confirmed an impaired LV systolic function with akinetic mid and apical segments and hyperkinetic basal segments (Fig. 2). The cardiac ultrasound showed typical apical ballooning (Fig. 3). The troponin level was elevated to 3 mg/L. An optimal medical treatment including beta-blockers and angiotensin converting enzyme-inhibitors were initiated. The patient evolved well clinically, the ECG normalized with disappearance of ischemic ECG changes and the control cardiac ultrasound at day six showed a total recovery with a normal LV function.
Discussion
TTC, also known as transient LV apical ballooning syndrome or stress-induced cardiomyopathy, is a reversible cardiomyopathy mimicking acute myocardial infarction, usually precipitated by acute physical or emotional stress and most commonly affects postmenopausal women.1) The exact physiopathology of TTC remains unclear. Catecholamine-mediated cardiotoxicity is the most widely proposed mechanism given that patients typically present with a preceding history of extreme psychological and/or physical distress implying increased sympathetic activity with a direct catecholamine toxic effect on the cardiac myocytes.3)4) Furthermore, the syndrome is usually self limited and complete recovery can be achieved in two to three weeks. The growing number of clinical cases of TTC have demonstrated a wide field of possible etiologies beyond the emotional stress.
We report a case of a 67-year-old postmenopausal woman who was being supplemented by enteral feeding via a nasogastric tube and who developed TTC due to misdirection, probably favored by the mechanical blockade by the nasogastric tube, while swallowing the drug pills. It can be argued that misdirection in predisposed individuals may cause an acute stress resulting in increased sympathetic activity leading to this syndrome. In our patient, another potential causal mechanism could be cough-induced stress cardiomyopathy which has been previously reported.5)


 XML Download
XML Download