

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Early risk stratification is essential in the management of patients with suspected or confirmed acute coronary syndrome. Traditionally, risk stratification involves an evaluation of medical history, a physical examination, and electrocardiography (ECG) upon admission. In recent years, additional variables for early risk stratification in patients with ST elevation myocardial infarction (STEMI) have been identified, and include the elevation of cardiac biochemical markers. For example, the myocardial release of troponin I (TnI) and N-terminal pro-B-type natriuretic peptide (NT-proBNP) represent sensitive serum markers for minimal myocardial injury. When present, these markers are associated with an increased likelihood of a cardiac event.1) The elevation of another marker, high-sensitivity C-reactive protein (hsCRP), upon admission with STEMI is associated with an increased risk of complications both during hospitalization and after discharge.2) These biochemical markers are noninvasive indicators of the risk of first or recurrent cardiovascular events and also predict the success of therapeutic and preventive interventions.1) Thus, several studies have demonstrated the independent prognostic value of elevated TnI, NT-proBNP, or hsCRP at admission in patients with STEMI.3-9) Additionally, in patients treated for STEMI, early ST-segment resolution has been associated with a better outcome based on improved early infarct-related artery patency, smaller infarct size, and less impairment of left ventricular function.10-12)
However, the combination of these two early available tools for predicting risk soon after a patient's presentation has not been evaluated. To address these issues, we retrospectively assessed the clinical characteristics and follow-up outcomes of consecutive patients who received primary percutaneous coronary intervention (PCI) after STEMI. The aim of this study was to evaluate the combined effect of using multiple biochemical markers and ST-segment resolution assessments for early risk stratification in patients with STEMI and treated by PCI.
Subjects and Methods
Study participants
Between January 2006 and June 2008, 178 consecutive patients who presented with their first STEMI and were subsequently treated with primary PCI were enrolled in the study, which took place at two coronary care units at the Kyung Hee University Hospital, Seoul, Korea. All patients were treated according to the standard of care for STEMI and underwent primary PCI. The diagnostic work-up in all patients consisted of history, 12-lead ECG, blood chemistries, and a two-dimensional (2D) echocardiography. The inclusion criteria were as follows: 1) presentation within 12 hours of symptom onset; 2) chest pain lasting ≥30 minutes and resistant to nitrates; and 3) ≥0.2 mV ST-segment elevation in at least two contiguous leads on 12-lead ECG. The exclusion criteria were as follows: 1) prior myocardial infarction, defined by pre-existing pathologic Q-wave; 2) non-ST elevation myocardial infarction; and 3) thrombolytic therapy taken instead of PCI. Patents with infectious disease, collagen disease, malignant disease, or severe hepatic or renal failure were also excluded. Initial clinical demographic data, including Killip classification, symptom-to-balloon times, door-to-balloon times, and pre- and post-thrombolysis in myocardial infarction (TIMI) flow grades were evaluated. All patients included in the study sample provided written informed consent for all procedures and our institutional review board approved this research.
Electrocardiographic and echocardiographic assessment
For all 178 patients, a standard 12-lead ECG was obtained at initial presentation and at 60 minutes after PCI, and was obtained by investigators blinded to the clinical characteristics and coronary angiography findings of the patients. Using calipers, the sum of the ST-segment elevation 20 ms after the J point was calculated and compared with the baseline ECG. The percent resolution of the ST-segment on ECG was categorized as complete (≥70%), partial (30% to 70%), or incomplete (≤30%), as originally described by Schroder et al.10) In all patients, standard echocardiography was performed within one hour after coronary intervention. Left ventricular (LV) ejection fraction (EF) was also assessed.
Biochemical markers
Blood samples used to obtain serum levels of TnI, NT-proBNP, and hsCRP were taken on presentation at the emergency department of each center. Creatine phosphokinase (CK), CK-MB isoenzyme, and TnI levels were measured quantitatively at admission, six hours later, and then twice daily over the first 48 hours. Levels were detected routinely in the laboratory using commercially available assays (Abbott Immunoassay, Abbott Laboratories, Abbott Park, IL, USA). The normal value of TnI in our institution is 0.5 ng/mL. TnI levels ≥0.5 ng/mL on admission was used as a serum marker for myocardial ischemia. NT-proBNP and hsCRP levels were also measured quantitatively at admission. NT-proBNP was quantified using a one-step enzyme immunoassay based on electrochemiluminescence technology (Elecsys 2010, Roche Diagnostics). Finally, hsCRP was determined with the Hitachi 717 system (Roche Diagnostics).
Follow-up and end points
All study participants underwent the implantation of drug-eluting stents (DES). The choice of the specific type of DES {i.e., sirolimus-eluting (Cypher, Cordis, Johnson & Johnson, Miami Lakes, FL, USA) or paclitaxel-eluting (Taxus, Boston Scientific, Natick, MA, USA) stents} was left to the surgeon's discretion. Patients were prescribed aspirin and clopidogrel for at least six months, regardless of DES type. All participants were followed for at least six months (13.6±3.1 months). The outcome events in this study were all cause mortality, repeated myocardial infarction, and readmission for worsening of heart failure up to six months after PCI.
Statistical analysis
Statistical analysis was performed using the SPSS package for Windows, Version 17.0. Continuous variables are presented as a mean±a standard deviation or median, as appropriate, and categorical variables as a percentage. Continuous data were compared using one-way analysis of variance among ST-segment resolution groups. Categorical data were compared using the chi-square test. Correlations between two continuous variables were performed using the Pearson correlation coefficient. A multivariate analysis using forward stepwise logistic regression was performed to check for independent variables related to major adverse cardiac events (MACE) reported up to six months of follow-up. The overall MACE-free survival rates were calculated using the Kaplan-Meier method, and the differences were determined using the log-rank test. The independent effects of variables on prognosis were calculated using a Cox proportional hazards regression model. Additionally, we performed a univariate and multivariate analysis using a Cox proportional hazards regression model, in which we explored the effects of different combinations of biomarkers on patient prognosis. A p<0.05 was considered statistically significant.
Results
Initial clinical characteristics in each ST-segment resolution group
The 178 patients treated with primary PCI were divided into the following three groups according to ST-segment resolution: complete (n=63, 59.9±12.3 years, male 81%), partial (n=90, 63.9±10.9 years, male 68%), and incomplete (n=25, 67.6±13.3 years, male 76%). Baseline characteristics, risk factors, LV EF, and biochemical markers at admission are listed in Table 1. Patients in the incomplete resolution group were older, had worse Killip classifications, and had significantly prolonged symptom-to-door times and door-to-balloon times. Risk factors such as diabetes, hypertension, dyslipidemia, smoking history, and ischemic heart disease history were not different among the three groups. There were no significant differences among the groups regarding use of medications, such as aspirin, clopidogrel, beta-blockers, angiotensin converting enzyme inhibitors, angiotensin receptor blockers, and statins either during admission or after discharge (data not shown).
Laboratory and echocardiographic findings in each ST-segment resolution group
The LV EF was significantly lower in patients with incomplete resolution (Table 1). Biochemical markers, such as TnI, NT-proBNP, and hsCRP at admission were significantly higher among patients in the incomplete resolution group, and were well correlated with the percent of ST-segment resolution (r=-0.38, p<0.01; r=-0.41, p<0.01; r=-0.43, p<0.01, respectively). However, the maximal values of CK-MB and TnI after PCI were not significantly different among the three groups (data not shown).
Angiographic findings and clinical outcomes
As shown in Table 2, there were no differences among the 3 groups in the number of diseased vessels, location of the culprit artery, type of lesion, or target lesion. Pre- and post-TIMI flow grade 0 or 1 was more commonly observed in the incomplete group, but this finding was not statistically significant. The duration of coronary care unit admission in days was significantly prolonged in the incomplete group (2.3±1.4, 3.2±2.3 and 4.7±2.9, respectively; p<0.05). Three (1.7%) patients died before discharge, and another four (2.2%) patients died during the follow-up period. The in-hospital mortality was only in the incomplete group.
The all-cause mortality rate increased stepwise according to ST-segment resolution status (0%, 1%, and 24%, respectively; p<0.01). Three patients were retreated due to repeated infarction, as shown in Table 2. During follow-up, 17 patients were readmitted for worsening congestive heart failure. The readmission rate was 3% (2/63), 10% (9/90), and 24% (6/25) in complete, partial, and incomplete ST resolution groups, respectively (p<0.01).
Prognostic values of biochemical markers and ST-segment resolution
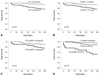
Using median values, the study sample was divided into two groups according to the initial TnI (median=0.38 ng/mL), hsCRP (median=2.45 mg/L), and NT-proBNP (median=456 pg/mL) levels. Kaplan-Meier curves showing MACE-free-survival based on the biochemical levels and ST-segment resolutions are presented in Fig. 1. There was a significant increased risk of six-month MACE with increasing baseline circulating levels of either TnI (6%, and 23% for lower and higher levels, respectively; p<0.01), hsCRP (6%, and 23% for lower and higher levels, respectively; p<0.01), or NT-proBNP (10%, and 24% for lower and higher levels, respectively; p<0.05). There was also a significant, gradually increased risk of six-month MACE according to the ST resolution status (5%, 12%, and 48% for complete, partial and incomplete ST resolution, respectively; p<0.01).
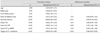
To evaluate the independent contribution of ST-segment resolution to the prediction of clinical outcomes after STEMI, multiple regression analysis was performed (Table 3). Variables used for this analysis were age, Killip classification, symptom-to-balloon time, door-to-balloon time, LV EF, TnI, hs-CRP, NT-proBNP, and the degree of ST-segment resolution. For multiple regression analysis, univariate analysis was selected for factors showing a p<0.05. The most important predictors of clinical outcomes after STEMI were the LV EF {hazards ratio (HR): 0.83 (0.76-0.91), p<0.01}, hsCRP {HR: 1.15 (1.05-1.26), p<0.05}, and the degree of ST-segment resolution {HR: 0.96 (0.93-0.09), p<0.05}. The additional benefit of using ST-segment resolution to predict cardiac events is shown in Fig. 2. With regard to the incremental value, ST-segment resolution is a good parameter to predict MACE after STEMI. However, the addition of biochemical markers markedly improved the prognostic utility of the model containing ST-segment resolution.
Discussion
In this study, initial TnI, NT-proBNP, and hsCRP plasma levels were higher in the incomplete ST-segment resolution group than in the ST-segment resolution groups, and these elevated biomarkers on admission predicted an adverse prognosis over the following six months, especially among patients who presented with two or three elevated biomarkers. Furthermore, biochemical markers, such as TnI, NT-proBNP, and hsCRP at admission were well correlated with the percent of ST-segment resolution. The combination of these tools improved risk stratification in STEMI.
In agreement with previous studies,13-15) elevated levels of TnI, NT-proBNP, and hsCRP were each associated with higher rates of MACE. Among them, only the hsCRP at initial presentation was significantly and independently associated with an adverse prognosis over the next six months. This finding suggests that the inflammatory process associated with myocardial necrosis may be still ongoing when the degree of inflammation in the acute phase increases, as several lines of studies have suggested.16-18)
By contrast, TnI and NT-proBNP were not independent predictors of clinical outcomes. This discrepancy with previous studies is probably explained by the relatively small sample size. However, despite the small sample size, the combination of several these markers allowed for a very good prediction of clinical outcomes in patients with STEMI treated with PCI as shown in Fig. 2. These incremental effects could be explained by the different pathophysiological mechanisms assessed by these three biomarkers in myocardial ischemia, i.e., elevations in troponins indicate myocardial necrosis,3)13) NT-proBNP is elevated in response to left ventricular overload,8)9) and hsCRP is a marker of inflammation.1)2) Multi-marker approaches to rapidly stratify patients and identify those at risk for adverse cardiac outcomes may help in the selection of more intense interventional or pharmacological treatment strategies.
In the present study, ST-segment resolution at 60 minutes was independently associated with six-month MACE, which agrees with the findings of previous studies.3)10) Another strong finding was a positive correlation between ST-segment resolution and the three biochemical makers. We evaluated the association between the initial biochemical makers and partial or incomplete ST-segment resolution. In a multivariate analysis, elevated hsCRP {HR: 6.29 (2.43-16.30), p<0.01} and elevated NT-proBNP {HR: 3.32 (1.29-8.52), p<0.01} were independently associated with partial or incomplete ST-segment resolution, but not elevated TnI {HR: 2.47 (0.99-6.20), p=0.053}. This finding suggests that high burdens of inflammation and ventricular loads may be associated with a lower likelihood of successful epicardial reperfusion. For this reason, the combination of biomarkers and early ST-segment resolution improved risk prediction. Biomarkers at admission and ST-segment resolution at 60 minutes are strong predictors of clinical outcomes, and the combination of them gives additive early information concerning patient prognosis, and further improves risk stratification in STEMI.
There are several limitations to the present study. Only a small number of patients from two centers were enrolled. The possibility of selection bias and low statistical power must therefore be considered when interpreting our findings. However, we demonstrated that elevated levels of biochemical markers were each associated with higher rates of clinical outcomes, as has been demonstrated by previous studies.1)7)11)15) We also showed the powerful prognostic value of the combination of biomarkers at admission and ST-segment resolution at 60 minutes.
Another weak point of this study is that it was a retrospective study and we therefore could not control medications use. In this study, medications were chosen by each physician according to each patient's status. Nevertheless, there was no significant difference in medication use among the three groups. We also achieved the purpose of this study by demonstrating improved predictions of clinical outcomes using the two different systems for patients with first STEMI.
Conclusion
Our study suggests an association among high plasma levels of TnI, NT-proBNP, and hsCRP at admission, incomplete ST segment resolution in patients with STEMI after PCI, and unfavorable clinical outcomes. Multi-directional approaches to risk stratification and treatment of patients with ST-EMI may improve the outcomes of adverse cardiac events.



 XML Download
XML Download