

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The precise recognition of the anatomy and physiology of coronary arteries is becoming increasingly important in coronary interventions. The primary disadvantages of intravascular ultrasonography (IVUS) being used routinely in a cardiac catheterization laboratory are its high expense and lengthy procedure time. However, IVUS has the unique ability to visualize atherosclerotic plaques on the vessel wall,1) guide stent implantation, improve proper deployment, and avoid the risk of stent thrombosis and related complications.2) In this paper, we report on the case of a crushed coronary stent caused by IVUS catheter entrapment.
Case
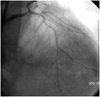
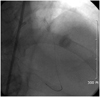
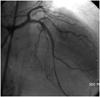
An 80-year-old man had a sudden onset of chest pain lasting 11 hours. He had a history of hypertension and 60 pack years smoking. The electrocardiographic (ECG) showed an ST segment depression of V 4-6 leads. Coronary angiography (CAG) showed significant narrowing and severe calcification of the distal left main coronary artery and middle left anterior descending (LAD) artery (Fig. 1). Successful percutaneous coronary intervention (PCI) was performed with stent implantation overlapping Coroflex Blue stent (2.75×25 mm, 2.75×29 mm, B. Braun Melsungen AG, Melsungen, Germany) (Fig. 2). One week later, the patient complained of further chest pain. Urgent CAG was performed and showed total occlusion of the middle LAD artery (Fig. 3). The aspiration of thrombi was performed successfully using a thrombuster catheter (3.9 Fr, Kaneka, Japan) (Fig. 4). In order to examine causes of acute stent thrombosis such as inadequate stent expansion and distal dissection, the IVUS catheter (2.5 Fr, 30 MHz, Boston Scientific, Natick, USA) was inserted into the vessel with ease. IVUS imaging showed adequate stent strut apposition and expansion but the IVUS catheter was stuck on the wire (0.014 inch, 180 cm, Seto, Aichi, Japan). Even though the IVUS catheter was returned to its original position, the inserted stent was damaged, and the middle LAD artery was consequently dissected. After several maneuvers to free the tip of the IVUS failed, both the guidewire and IVUS catheter had to be removed by strong manual traction, simultaneously (Fig. 5). After we tried several attempts to pass the wire into the distal true lumen through the crushed stent in the middle LAD, we were able to pass the wire into the central portion of the distal true lumen with Thrombolysis in Myocardial Infarction 2 flow. However, the sprinter balloon (1.25×6 mm, Inc. Minneapolis, MN, USA) could not pass the crushed stent using the anchor balloon technique. We attempted to pass the wire across the lateral side before the stent collapsed in a major way (Fig. 6). The sprinter balloon was passed through the crushed stent, and PCI was performed using a sequential large balloon. Another longer and thinner stent (2.5×28 mm, B. Braun Melsungen AG, Melsungen, Germany), was successfully implanted with higher pressure (18 atm) (Fig. 7). After the stent was inserted, no further IVUS examination was done. After 4 days, the patient was discharged with aspirin and clopidogrel medications, and no symptoms or ECG change was observed.
Discussion
IVUS provides a unique perspective on viewing vascular disease and intervention effects. As a complement to coronary angiographies, IVUS has the ability to analyze vessel wall morphology in vivo, accurately displaying vessel structure detail and tissue characterization, providing critical information like the presence and degree of calcified plaques and quantification of luminal dimensions. It also permits the characterization of the composition of stenotic lesions into soft plaques, hard plaques, calcification, and types of thrombus.3)
IVUS itself may be associated with serious procedural complications such as dissection, acute vessel closure, embolism, thrombus, and the need for urgent bypass surgery, which occurs in less than 0.5% of cases.4) The role of IVUS after stent placement remains debatable. Although acute luminal gain may be greater with IVUS guidance, long-term benefits are yet to be clearly demonstrated.5)
An IVUS study was interrupted in 2,207 patients due to technical failures experienced in 6 patients with guidewire winding and in 3 patients with broken catheters.6) Guidewire entrapment occurred twice when the distal portion of the catheter advanced over the flexible portion of the guidewire. One report demonstrated severe stent damage after IVUS catheter pullback.1) Another report observed four cases of wire kinking by the use of IVUS catheter and pressure wire simultaneously.7) Yet another case described 4 patients in whom the distal tip of the pressure wire was entrapped during an IVUS examination and 3 patients experienced transient angina.7) The above cases were resolved by torquing the catheter along with a gentle forward movement over the wire or making a small loop of wire before entering the crushed stent strut, which may prevent the wire from becoming entangled across the stent struts. Since the looping wire tip increases its cross sectional diameter, it is possible to avoid entering the false lumen created by balloon angioplasty.
In our case, the crushed stent was caused by IVUS entrapment. Fortunately, the wire across the lateral side and ballooning before the stent collapsed. If these techniques out of the entry are unsuccessful or if ischemia occurs, surgical extraction of the fragment or bypass surgery would be necessary. Careful observation is required, and the prolonged use of systemic anticoagulation may be necessary if the crushed stent can not be removed. In this situation, forceful withdrawal of the catheter may result in separation of the IVUS catheter tip entrapment.
To avoid these situations and assess the risk, we considered the location and status (e.g., calcification) of blood vessels before IVUS insertion. In addition, IVUS can be thought of ways to reduce the diameter and the development of this technology is thought to be resolved while. In our study, IVUS examination of a rare complication was used in the diagnosis.




 XML Download
XML Download