

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Kawasaki disease (KD) is an acute, self-limited vasculitis that affects mainly infants and young children.1)2) Ten to fifteen percent of patients with untreated KD develop coronary arterial lesions.3-5) Although it has been shown that coronary complications can be significantly reduced by the use of high-dose intravenous immunoglobulin (IVIG) therapy combined with oral acetylsalicylic acid, the etiology of KD still remains unknown.6)
KD is known to involve an immune-mediated inflammatory process that leads to endothelial cell damage.7) The immunological changes in KD are evidenced by an increase in serum levels of cytokines, such as tumor necrosis factor (TNF)-α, interleukin (IL)-1, IL-2, IL-6, and interferon (IFN)-γ during the acute phase.8)9) The stimulus for increased serum levels of cytokines remains unknown.
Polymorphisms in genes encoding these crucial immunomodulatory molecules may result in an altered level of expression, and hence must be considered important candidate genes for KD susceptibility and disease severity. The genetic susceptibility to specific diseases may be identified by considering several genetic variants together.
IL-6 is a pro-inflammatory cytokine secreted by T cells and macrophages to stimulate an immune response leading to inflammation.10) It is associated with atherosclerosis and myocardial infarction11) and is one of the most important mediators of fever and of the acute phase response. Serum IL-6 during the acute phase showed a significant correlation with the duration of fever in patients who were not treated with IVIG. This suggests that the regulation of IL-6 expression in KD patients may differ from that in normal children, possibly due to gene polymorphisms.12) However, there are controversies about the association between the IL-6 gene polymorphism and development of KD. Therefore, we studied the possible genetic influence on the expression of IL-6 in KD patients by examining serum levels of IL-6 and the IL-6 (-636 C/G) gene polymorphism.
Subjects and Methods
The study group included 189 KD patients (108 males and 81 females) with a mean age of 40.5 months from the Department of Pediatrics at Ewha Womans University Hospital and the Asan Medical Center, Seoul, Korea. The subjects were all Koreans born in Seoul.
All of the KD patients were treated with IVIG (2 g/kg/day for 1 day), and oral aspirin (50 mg/kg/day). Echocardiography was performed by pediatric cardiologists to detect the presence of coronary artery lesions prior to IVIG administration. Coronary arteries were defined as abnormal if the internal lumen diameter was >3 mm in children younger than 5 years old and >4 mm in children 5 years old or more; if the internal diameter of a segment measured ≥1.5 times that of an adjacent segment; or if the coronary lumen was clearly irregular.13) The control group consisted of 191 children (88 males and 103 females) aged 29.0 months on average, with congenital heart disease which included ventricular septal defect (n=64), Tetralogy of Fallot (n=61), patent ductus arteriosus (n=33), atrial septal defect (n=20), total anomalous pulmonary venous return (n=7), and interrupted aortic arch (n=6).14) None of the patients had congestive heart failure.
Laboratory data were obtained from each child, including complete blood count (CBC), erythrocyte sedimentation rate (ESR), platelet count, alanine aminotransferase (ALT), aspartate aminotransferase (AST), serum total protein, albumin, and Creactive protein (CRP). Genomic DNA samples were extracted from their peripheral bloods before IVIG therapy in the KD patient group and before operation for their congenital cardiac abnormalities in the control group.
The study was carried out with the approval of the ethics committee of Ewha Womans University Hospital and the Asan Medical Center Institutional Review Board, and written informed consents were obtained from the parents of all subjects.
Genotyping of the interleukin-6 (-636 C/G) gene polymorphism
The genomic DNA was prepared from peripheral blood. The IL-6 (-636 C/G) single nucleotide polymorphism (rs180 0796) was genotyped by using the single base extension method. PCR was performed in reaction mixtures containing 1.25 pmol of each primer (sense, 5'-AGGATGGCCAGGCAGTTC-3' and antisense 5'-CCAGTCATCTGAGTTCTTCTGTGTT-3'), 50 ng of genomic DNA, 250 mM dNTPs, and 0.15 U Taq DNA polymerase (Applied Biosystems, Foster City, CA, USA) in the buffer provided by the manufacturer. Amplification was performed in a GeneAmp PCR System 9700 thermal cycler (Applied Biosystems).
To clean up the PCR products for the primer extension reaction, each reaction mixture was incubated with 1 U of shrimp alkaline phosphatase (SAP; Amersham Life Sciences, Cleveland, OH, USA) and 2 U of Exol (Amersham Life Sciences) for 1 hour at 37℃, and then at 72℃ for 15 minutes for enzyme inactivation. Primer extension reactions were performed with a SNaP Shot ddNTP Primer Extension Kit (Applied Biosystems), according to the manufacturer's instructions. The primer extension reaction products were cleaned up by incubation at 37℃ for 1 hour in the presence of 1 U of SAP, followed by incubation at 72℃ for 15 minutes. The extension products were then mixed with the Genescan 120 Liz size standard solution (Applied Biosystems) and Hi-Di formamide (Applied Biosystems), incubated for 5 minutes at 95℃, placed on ice for 5 minutes, and then electrophoresed on an ABI Prism 3100 Genetic Analyzer (Applied Biosystems). The results were analyzed by using the ABI Prism GeneScan and Genotyper software packages (Applied Biosystems).
Measurement of serum IL-6
Serum samples were obtained from KD patients and control subjects. Venous blood was withdrawn in the acute febrile stage before IVIG treatment in KD patients. Serum IL-6 levels were measured by using a sandwich enzyme immunoassay-based Quantikine Human Interleukine-6 kit (R&D systems Inc., Minneapolis, MN, USA), according to the manufacturer's instructions.
Statistical analysis
Statistical Package for the Social Sciences (SPSS) 12.0K for Windows (SPSS Inc., Chicago, IL, USA) was used for all statistical analyses. Clinical characteristics, including CBC, ESR, platelet counts, ALT, AST, serum total protein, albumin, CRP, and total duration of fever were analyzed as a quantitative trait. Differences in clinical phenotypes between groups were analyzed using the Mann-Whitney U-test.
Unconditional logistic regression analysis adjusted for age and sex was used to calculate adjusted odds ratios (aOR), 95% confidence intervals (CI). A p<0.05 was considered statistically significant.
Results
Clinical characteristics of study subjects
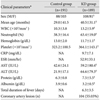
Clinical characteristics are shown in Table 1. White blood cell (WBC) count (neutrophil), platelet count, ALT, AST, and total protein were significantly higher, and hemoglobin and albumin levels were significantly lower in the KD group compared with the control group (p<0.05). Coronary arterial lesions in the KD group were noted in 104 patients (55.03%).
Allele frequencies of the interleukin-6 (-636 C/G) polymorphism in the Kawasaki disease group and the control group
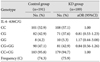
The 189 study subjects and 191 patients in the control group were genotyped for the IL-6 (-636 C/G) polymorphism, and allele frequencies were examined. The genomic frequencies of the IL-6 (-636 C/G) polymorphism in the KD group were 57.1% (108/189) for CC, 37.6% (71/189) for CG, and 5.3% (10/189) for GG. In the control group, these frequencies were 52.9% (101/191) for CC, 42.9% (82/191) for CG, and 4.2% (8/191) for GG. The genotype frequencies of these samples were in accordance with Hardy-Weiberg equilibrium. The genomic and allelic frequencies of this polymorphism did not significantly differ between the KD group and the control group (Table 2).
Association between the interleukin-6 (-636 C/G) polymorphism and clinical parameters in the Kawasaki disease group and the control group
Clinical parameters were compared between the KD group and the control group according to allele frequencies. WBC count (neutrophil), platelet count, AST, ALT, and total protein were significantly higher in the KD group compared with the control group. Interestingly, albumin concentrations were significantly lower in patients with KD with -636 C/G and those with GG genotypes, compared to those with the CC genotype (Table 3).
Allele frequencies of the interleukin-6 (-636 C/G) polymorphism in Kawasaki disease children with and without coronary arterial lesions
We determined whether the IL-6 polymorphism was associated with coronary arterial lesions in children with KD. In the KD group without coronary arterial lesions, allele frequencies were 54.2% (45/83) for CC, 39.8% (33/83) for CG, and 6.0% (5/83) for GG. In the KD group with coronary arterial lesions, allele frequencies were 59% (59/100) for CC, 37% (37/100) for CG, and 4% (4/100) for GG. There was no difference in the IL-6 (-636 C/G) polymorphism according to coronary arterial lesions (Table 4).
Serum interleukin-6 levels in the Kawasaki disease group and the control group
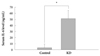
Serum IL-6 concentrations were 2.72±6.49 ng/mL in the control group and 51.0±13.85 ng/mL in the KD group. Serum IL-6 concentrations were markedly elevated in the KD group compared with the control group (Fig. 1).
Serum interleukin-6 levels in the Kawasaki disease group with CC and CG+GG genotypes
The serum IL-6 concentration was examined according to genotype. Serum IL-6 levels were 21.0±23.4 ng/mL in patients with KD who had the CC genotype and 69.3±30.9 ng/mL in patients with the -636 C/G and those with the GG genotype (Fig. 2).
Discussion
The etiology for KD remains unknown, but several studies have suggested the involvement of an immune-mediated process. Cytokines such as IL-1, IL-6, IFN-γ, TNF-α are released inducing a series of inflammatory reactions leading to endothelial cell injury and inflammation of small and medium-sized arteries, especially coronary arteries.15-17) Cytokines with polymorphic gene sequences are potential markers of disease susceptibility.15)16)
In recent years, it has been well demonstrated that inflammatory molecules, as well as single nucleotide polymorphisms of genes encoding inflammatory mediators, may contribute to the development and progression of a large number of pathologic conditions including cardiovascular disease.18-21)
One commonly used technique to identify genetic risk factors for multifactorial diseases such as KD is the candidate gene approach, which directly examines the effects of genetic variants of a possibly contributing gene by an association study. To date, quite a number of genes have been examined, which are usually selected based on information regarding their function in inflammation, the immune response, and other biological mechanisms.18)
Single nucleotide polymorphisms (SNP) of pro-inflammatory and anti-inflammatory genes may strongly influence the plasma levels and biological activity of the corresponding proteins, with potentially important clinical implications.22)23)
Burns et al.24) reported that the genetic variation in the IL-4 gene or regions linked to IL-4, plays an important role in KD pathogenesis and disease susceptibility. Jin et al.25) reported that the IL-10 (-627 A/C) gene polymorphism may be associated with coronary aneurysms and low albumin in Korean children with KD. IL-6 expression was noted in several diseases such as systemic lupus erythematosus,26) sporadic Alzheimer's disease,27) and systemic onset juvenile chronic arthritis.28)
The IL-6 gene -174G>C and -572G>C gene polymorphisms are associated with cerebral aneurysm.28) Whether this association is due to the development, progression, or rupture of such an aneurysm or represents survivor bias is unclear. Sohn et al.29) examined the IL-6 gene polymorphism at +162 bp, +168 bp and -594 bp, and reported that the polymorphism was not associated with KD. In KD, IL-6 has been reported to rise more than any other cytokine and correlates with coronary complications.15)
There have been no reported studies about the association between the IL-6 (-636 C/G) polymorphism and KD. In this study, we investigated the association between the IL-6 (-636 C/G) polymorphism (rs1800796) and KD. The IL-6 (-636 C/G) polymorphism showed no difference in gene frequency between the KD group and the control group. There was no difference in the IL-6 (-636 C/G) polymorphism according to coronary arterial lesions either. Nonetheless, the serum IL-6 levels were significantly higher in the KD group than the control group and among the KD group, serum IL-6 levels were significantly higher in the CG+GG group compared to the CC group. Likewise, albumin concentrations were significantly lower in the KD group than the control group and among the KD group, the CG+GG group showed lower levels than the CC group. Therefore, our findings suggest that the IL-6 (-636 C/G) polymorphism may be associated with risk factors of KD, such as a low albumin concentration. In addition, elevated serum IL-6 concentrations in the CG+GG genotype suggests the possibility of a relationship between the IL-6 (-636 C/G) polymorphism and KD that needs to be analyzed further.
Our studies have some limitations. The studied population is relatively small in number. We enrolled patients with congenital heart disease as a control group instead of normal children. Also there is a possibility of linkage disequilibrium with an unknown risk single nucleotide polymorphism and the lack of function-related experiments. There have been no reported studies on the relationship of the transcription activity of IL-6 in KD. SNPs on the IL-6 promoter could affect the transcription activity and furthermore the expression of IL-6. Such SNPs could be a good candidate marker to study the transcriptional activity of IL-6.
In conclusion, we found that the IL-6 (-636 C/G) polymorphism was not associated with the development of KD or coronary arterial lesions. This study suggests however, that the IL-6 (-636 C/G) polymorphism might prove useful as a genetic marker for the indicators of KD such as duration of fever, platelet count, and albumin concentration. Given the limitations of our study, it is not possible to definitely rule out the direct correlation between the IL-6 (-636 C/G) polymorphism and KD. Further large scale studies will be needed to establish the relationship between IL-6 gene polymorphisms and KD.



 XML Download
XML Download