

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Pneumopericardium is defined as the presence of air-fluid level in the pericardial sac and has been reported to result from a spontaneous or iatrogenic cause of underlying disease.1) It is a rare condition but is important in the differential diagnosis of chest pain. Posteroanterior chest radiographs typically reveal air-fluid level and a radiolucency of air surrounding the cardiac boarder is outlined by a fine line representing the pericardial sac. Although severe complications occur in some patients, the iatrogenic pneumopericardium is self-limiting and requires no specific therapy.2) We discuss a case of iatrogenic pneumopericardium in a young man who underwent pericardiocentesis due to tuberculous pericardial effusion.
Case
A 20-year-old man was referred to the hospital with extensive pericardial effusion on a computed tomography. The patient had a history of pulmonary tuberculosis for 2 years and had taken anti-tuberculosis medication for the past 8 months. Physical examination showed stable vital signs: blood pressure, 131/65 mmHg; pulse rate, 92 bpm; respiratory rate, 26 per minute; body temperature, 36.5℃.
Posteroanterior chest radiographs showed cardiomegaly without any lung lesion (Fig. 1). An emergent echocardiogram showed a large circumferential pericardial effusion and diastolic right atrium collapse without respiratory variation of the mitral inflow. The left ventricular ejection fraction was estimated to be 60%. A 7Fr ARROWgard Blue® catheter (Arrow International Inc, Bernville, PA, USA) was used for subxiphoid pericardiocentesis. Over 1,000 mL of serous fluid was drained from the pericardial sac over the following 12 hours. Subsequently, the patient's resting dyspnea was resolved. Sputum and pericardial fluid cultures and smear for AFB and other organisms were negative. The pericardial fluid was a lymphocyte dominant exudate, containing protein 6.5 g/dL, albumin 3.6 g/dL, lactate dehydrogenase 466 U/L and white blood cell 7,200 cells/µL (lymphocyte 84%). Polymerase chain reaction for Mycobacterium tuberculosis deoxyribonucleic acid was negative with pericardial fluid and adenosine deaminase in pericardial effusion was 96 IU/L (normal, 5 to 23 IU/L) (Fig. 2).3)
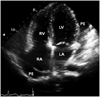
On day 5 after the pericardiocentesis the patient developed a pleuritic chest pain. His blood pressure was 110/70 mmHg, heart rate was 72 bpm, and respiratory rate was 20 per minute. Follow up chest radiographs showed a new lucent outline around the heart with a clear lung, representing the existence of air-fluid level in the pericardial space (Fig. 3). Echocardiography revealed scanty pericardial effusion, a bright echogenic spot swirling in the pericardial cavity and an absent tamponade (Fig. 4).
Discussion
Pneumopericardium is a rare complication of pericardiocentesis. The diagnosis of pneumopericardium can be made by conventional chest radiographs, CT, or echocardiography.5) In posteroanterior chest radiographs, a continuous thin radiolucent rim of air and air-fluid level follows the cardiac silhouette and is outlined by a fine line representing the pericardial sac.2) Pericardiocentesis with extended catheter drainage is a safe treatment for managing clinically significant pericardial effusions and can be performed effectively under local anesthesia.6) The subxiphoid window should be the standard initial procedure in most patients requiring drainage for effusive pericardial disease. It is less morbid than the transthoracic approach and allows a shorter hospital stay.7)
For our patient we hypothesized that pneumopericardium was induced by chance due to forced coughing during drainage after pericardiocentesis. In tension pneumopericardium, rapid fluid resuscitation and emergent echo-guided pericardiocentesis, followed by pericardial drainage, should be performed. If the hemodynamic condition is stable, the underlying condition should be treated and the patient should be monitored closely.2) The patient was in a tolerable state, so we treated him conservatively and removed catheter drainage.
The current case showed that pneumopericardium is a rare complication of pericardiocentesis, which occurs as a result of a leaky drainage system or direct pleura-pericardial communication.




 XML Download
XML Download