

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The efficacy of 3-hydroxy-3-methylglutaryl-coenzyme A reductase inhibitor (statin) in reducing cardiovascular events has been established in many large-scaled randomized controlled trials.1)2) In addition to their potent effects on cholesterol levels, statins influence several other pathways, including the inflammatory, oxidative, and thrombotic processes.3-5)
The inflammatory processes are not only involved in the pathogenesis of atherosclerosis but also in the cause of acute coronary syndromes.6)7) High levels of C-reactive protein (CRP), a prototype inflammatory marker, are associated with increased cardiovascular disease risks.8)9)
Many studies have shown that statins reduce CRP levels.10)11) However, it is unclear whether the anti-inflammatory effect of statin is mediated by cholesterol reduction per se, or through direct mechanisms, the so called pleiotropic effects, as previous generations of lipid lowering drugs did not have comparable potency that of the statins.
A new drug, ezetimibe, inhibits the intestinal absorption of cholesterol by impeding cholesterol transport across the intestinal wall, and lowers cholesterol levels by over 15%.12-15) Ezetimibe alone does not reduce CRP levels. However, several reports have suggested that ezetimibe might potentiate the effect of statin on CRP level when administered together.14)15) A study reported that the addition of ezetimibe to patients taking statins decreased CRP levels.16) In contrast, several reports have suggested that cholesterol reduction by ezetimibe failed to demonstrate the pleiotropic effects of statins.17-19)
The aim of this study was to investigate the effect of ezetimibe on CRP levels when administered to hypercholesterolemic patients already receiving statins, and to evaluate the relationship between the cholesterol reduction and anti-inflammatory effects.
Subjects and Methods
One hundred-seventy and nine (n=179) hypercholesterolemic patients were enrolled. The exclusion criteria were: 1) new onset diseases that potentially impact on lipid levels, such as diabetes mellitus, infectious diseases, or other endocrinologic diseases, within 3 months, 2) aspartate aminotransferase (AST) or alanine aminotransferase (ALT) levels ≥3-fold the upper normal limit, 3) administration of medications within the last 3 months that might affect lipid levels, and 4) baseline CRP levels ≥10 mg/L. One hundred-twenty (n=120) hypercholesterolemic patients receiving statins required additional reduction of low density lipoprotein-cholesterol (LDL-C) to meet the target levels of the National Cholesterol Education Program were divided into two groups, the ezetimibe group (10 mg of ezetimibe, n=60) and the control group (n=60).20) A patient in the ezetimibe group was excluded in the analysis, because follow-up CRP level was over 10 mg/L. A third group of hypercholesterolemic patients with similar baseline CRP levels and without statin therapy was enrolled and treated with statin (statin group, n=59).
CRP and lipid levels were measured before and after management for 2 months. After overnight fasting, blood samples were obtained. Concentrations of total cholesterol and trigly-ceride were determined by the enzymatic method using an automatic analyzer (Model 7150, Hitachi, Japan). LDL-C was calculated by the Friedewald equation. The concentration of high density lipoprotein-cholesterol (HDL-C) was measured by the direct method using immunoinhibition (Wako, Japan). The concentration of CRP was determined by the nephelometer method using an N High Sensitivity CRP kit (Dade Behring Marburg GmbH, Germany). Interassay coefficients of variation were 7.0% and 5.2% for the controls, with levels of 1.43 mg/dL and 1.74 mg/dL, respectively. The intra-assay co-efficient of variation was 1.5-3.0%.
Statistical analysis
Data are expressed as mean±SD. Statistical analysis was performed using the Social Package for the Social Sciences (SPSS Inc., Chicago, IL, USA). For CRP, lipoprotein (a) and triglyceride, the Wilcoxon signed-rank test was used to compare concentrations before and after therapy, and the Mann-Whitney U test was used to evaluate differences between groups. For other variables, a paired t-test was used to compare concentrations before and after therapy, and the Student t-test was used to evaluate differences between groups. Relationships between the parameters were analyzed by the Spearman correlation method. The distribution of discrete variables was analyzed using the χ2 test. A two-tailed p<0.05 was considered statistically significant.
Results
Baseline demographic and clinical characteristics were similar between the ezetimibe group and the control group (Table 1), except the number of patients with ischemic heart diseases (p=0.026). There were no differences in baseline lipid profiles and CRP levels between the ezetimibe group and the control group (Table 2). CRP levels were similar between the ezetimibe and the statin groups. However, LDL-C levels were higher in the statin group than in the ezetimibe group, due to different inclusion criteria (138.5±21.2 mg/dL vs. 172.9±28.4 mg/dL, p=0.000) (Table 2).
Ezetimibe decreased cholesterol and LDL-C levels by 20.2% (from 228.1±31.1 mg/dL to 182.1±25.6 mg/dL, p=0.000) and 28.1% (from 138.5±21.2 mg/dL to 99.6±20.0 mg/dL, p=0.000), respectively (Table 2). However, ezetimibe did not reduce CRP levels (from 0.83±0.68 mg/L to 1.14±1.21 mg/L, p=0.11). CRP levels did not change in the control group (p=0.42).
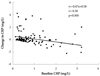
Changes in CRP levels were not associated with changes in LDL-C in the control (r=0.14, p=0.31), the ezetimibe (r=0.03, p=0.85), the control+ezetimibe (r=-0.02, p=0.87), and the statin groups (r=0.09, p=0.50) (Table 3). Changes in CRP levels were negatively associated with baseline CRP levels in the control+ezetimibe (r=-0.38, p=0.000) (Fig. 1), the control (r=-0.55, p=0.000), and the statin groups (r=-0.60, p=0.000), and in the ezetimibe group with borderline significance (r=-0.22, p=0.09). In the ezetimibe group, changes in CRP levels were negatively related to baseline HDL-C levels (r=-0.35, p=0.007). During the follow-up period, a patient in the ezetimibe group experienced elevation of AST and ALT ≥3-fold the upper normal limit. No patient experienced elevation of creatine kinase ≥10-fold the upper normal limit.
Discussion
This case-controlled study demonstrated that ezetimibe, a new cholesterol lowering drug, failed to decrease CRP levels in patients already taking statins, despite marked reduction in cholesterol and LDL-C levels. This finding suggests that cholesterol reduction itself does not modify the inflammatory processes, and that the anti-inflammatory effects of statins may not be secondary to lipid-lowering effect, but due to other pathways.
The present study had lower baseline CRP levels (0.82-0.84 mg/L) than previous studies (more than 2 mg/L).14-16) In the present study, changes in CRP levels were associated with baseline CRP levels. High baseline CRP levels predicted the decrease of CRP levels during the follow-up period. This finding is consistent with that of previous studies.21) Therefore, the difference in baseline CRP levels may explain the discrepancy between the present study and previous studies.
To exclude the effect of low baseline CRP levels, a third group of patients with similar CRP levels and without statin therapy were included. In these patients, statin lowered CRP levels. Therefore, lower baseline CRP levels alone cannot explain the difference between the present study and previous ones.
Ezetimibe did not reduce CRP levels.14)15) Several studies have suggested that the combined therapy of statin and ezetimibe may decrease CRP levels more so than statin monotherapy.14)15) However, as the primary aims of most previous studies focused on the drug's efficacy on lipid and safety, baseline CRP levels were different between the groups. In a study which evaluated the effect on CRP levels, baseline CRP levels were different by 12%.15) In the present study, baseline CRP levels were similar between the control and the ezetimibe groups.
The efficacy of the co-administration of ezetimibe on CRP levels may be different with the types or the dosage of statins. In general, the addition of ezetimibe to simvastatin (14.3-16.6%) was more effective than the addition of ezetimibe to atorvastatin (-0.3-10%).14)15)22-24) The addition of ezetimibe decreased CRP levels only in higher dose of statin in some studies14) or only in lower dose in other studies.22)
In a study which compared the effects on CRP between atorvastatin and simvastatin+ezetimibe, combined therapy failed to provide incremental reduction of CRP levels in spite of further reduction of LDL-C by 8.1%.22) Therefore, it is unclear whether co-administration of ezetimibe with statin potentiates the CRP lowering effect of statins.
There are two studies that assessed the effect of ezetimibe on CRP levels in patients already taking statins.16)25) In one study, addition of ezetimibe decreased CRP levels. However, baseline CRP levels were different by 23.5%.16) That study enrolled hypercholesterolemic patients having taken statins for 6 weeks and more.16) In the present study, almost all patients were taking statins over 12 months. In the JUPITER study, rosuvastatin in patients with elevated CRP levels reduced CRP levels from 4.2 mg/L to 2.2 mg/L after 12 months, and reduced further to 1.8 mg/L after 24 months.26) Therefore, difference in the duration of statin therapy may explain the discrepancy between these two studies. It is possible that the addition of ezetimibe to statin simultaneously or sequentially facilitate reduction of CRP levels without further reduction compared with the long-term statin therapy. Lower baseline CRP in the present study may partially be explained by the effects of long-term statin therapy.
In another study, the addition of ezetimibe to patients taking statins decreased CRP levels in Caucasian patients but not in African and Hispanic patients, although the difference did not reach statistical significance. As such, there is a possibility of ethnic difference.25)27) Recently, pooled data including the above two studies16)25) showed that addition of ezetimibe to patients taking statins decreased CRP levels.28)
Statins reduce cardiovascular events not only in hypercholesterolemic patients, but also in high-risk patients with normal or low cholesterol levels.1)2) It has been suggested that the cardioprotective effects of statins are mediated both by their potent effects on cholesterol levels and by other pathways, such as the inflammatory, oxidative, and thrombotic processes.3-5) Almost all reports have demonstrated that statins reduce CRP levels.10)11)
However, It is not known whether the pleiotropic effects of statins are mediated by cholesterol reduction per se, or by other mechanisms. It is because old cholesterol lowering drugs are not as potent as statins in reducing cholesterol levels. Ezetimibe lowers LDL-C by 16.9-18.7%.12-16) Its potency exceeds that of old cholesterol lowering drugs and is equivalent to earlier statins, lovastatin or pravastatin. These statins also lower CRP levels.10)11)
In the present study, ezetimibe did not decrease CRP levels in patients taking statins in spite of marked lowering of LDL-C levels by 28.1%. In addition, changes in CRP levels were not related to changes in LDL-C levels in all groups. This finding indicates that the anti-inflammatory effect of statin may not be secondary to cholesterol reduction.
Several studies have compared the effects on the pleiotropic mechanisms of cholesterol-reduction by ezetimibe with that by statins. Cholesterol reduction by ezetimibe, either as monotherapy or in addition to statins, failed to improve endothelial vasodilator function reduce platelet reactivity, oxidative stress, and inflammatory parameters.17-19) These findings are consistent with the results of the present study. Recently published studies are also consistent with the present study.29)30)
In the present study, changes in CRP levels were mainly associated with baseline CRP levels, and this finding is consistent with previous reports.21) In the ezetimibe group, CRP levels decreased in patients with lower baseline HDL-C levels and increased in those with higher baseline HDL-C levels (r=-0.35, p=0.007). In the control group, changes in CRP levels were negatively related to those in HDL-C levels with borderline significance (r=-0.24, p=0.063). This may have occurred as the inflammation processes decrease HDL-C levels.
This study has several limitations. The number of patients is smaller than that in previous studies. However, baseline CRP levels were well balanced in contrast to previous studies. As described above, lower baseline CRP levels may account for the difference between the outcomes of the present study and that of previous studies. This study was performed in a single hospital in Asia. The effect of ezetimibe may be variable between ethnic populations. Ischemic heart disease was more frequent in the ezetimibe group than in the control group, and this difference may influence the results.
In summary, ezetimibe failed to decrease CRP levels in patients taking statins in spite of marked reduction of total and LDL-C levels. Changes in CRP levels were not associated with that of LDL-C at all. Therefore, cholesterol reduction itself may not be able to reduce inflammatory processes in patients taking statins.



 XML Download
XML Download