

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Variant angina (also called Prinzmetal's angina) is characterized by spontaneous episodes of angina, especially in the morning, with ST segment elevation on the electrocardiogram.1) To diagnosis variant angina, the most common method is ergonovine provocation testing combined with a coronary angiogram.2-4) The diagnosis is positive if vasospasm and angina with change of ST segment is shown with ergonovine and returns to normal with nitroglycerin.5)6) This paper deals with a patient with vasospasm of the right coronary artery after ergonovine was injected, but ST elevation was not detected due to transient collateral circulation.
Case
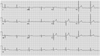
A 60-year-old man presented with a 2-year history of frequent chest pain. He had no specific past history including no history of hypertension or diabetic mellitus. He had smoked 1 pack of cigarettes per day for 40 years, and drank alcohol 2 times a week. His chest pain usually occurred in the morning, lasted about 30 minutes, and had no correlation to exercise. The pain would disappear without specific treatment. On admission, his blood pressure, pulse rate, respiratory rate and body temperature were 120/70 mmHg, 50 beats per minute, 12 per minute, and 36.6℃, respectively. There were no abnormal heart or respiration sounds. A laboratory examination showed that his troponin-I, creatine kinase-MB, total cholesterol, triglyceride, and high density lipoprotein-cholesterol were <0.2 ng/mL, 1.9 ng/mL, 173 mg/dL, 317 mg/dL and 28 mg/dL, respectively. An electrocardiogram on admission showed regular sinus rhythm without ischemic change (Fig. 1). The chest X-ray was also normal. An echocardiogram revealed normal left ventricular ejection fraction with normal valvular structure, but the basal inferior wall was hypokinetic.
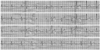
A diagnostic coronary angiography showed no abnormality or stenosis at the left anterior descending artery and its branch, but the left circumflex artery proper showed tubular eccentric of 30% stenosis (Fig. 2A). Afterwards, the right coronary artery was engaged and showed no abnormality or stenosis (Fig. 2B). Ergonovine provocation (100 µg of ergonovine) resulted in a complaint of chest pain similar to what the patient had been experiencing. A subsequent angiogram showed total occlusion at the proximal right coronary artery (Fig. 3B), but an electrocardiogram revealed no ST elevation or ST depression (Fig. 4). The left anterior descending artery and left circumflex artery was then engaged and was no stenosis, but a collateral artery was shown from the left descending artery to the right coronary artery (Fig. 3A).
Nitroglycerin was injected directly into the right coronary artery and the angiogram was taken again. The total occlusion of the proximal right coronary artery became normal (Fig. 5B). The angiogram of the left anterior descending artery and left circumflex artery angiogram was repeated, but the collateral artery that was shown at the right coronary artery spasm had disappeared (Fig. 5A).
The patient was treated with a calcium channel blocker and nitrate based on the diagnosis of variant angina.
Discussion
Variant angina is characterized by spontaneous episodes of angina particularly in the morning and with ST segment elevation on the electrocardiogram. The epidemiology of variant angina is 2-20% in Western population,7-9) and 4.4% in the Korean population.6) The mechanism of variant angina is unknown, but it is thought that a reduction of nitric oxide production and endothelial cell damage causes vasospasm induced by endothelial-derived relaxing factors and endothelial derived contracting factors.1) This vasospasm may also induce ischemia to the myocardium and the ST segment changes seen in the electrocardiogram. In studies by Feldman10) and Crea,11) 88% of patients presented ST segment changes and 12% had no ST segment change. The reasons given for no ST segment change at vasospasm were branch vasospasm, non total vasospasm, and 3-vessel vasospasm.10)11) All cases of total occlusion of vasospasm were detected by ST segment elevation.5)
In the case presented here, total occlusion of proximal right coronary was detected, but the electrocardiography showed no ST elevation. The reason was the appearance of a transient collateral artery from the left anterior descending artery to the distal right coronary artery at vasopasm. In spite of total occlusion due to vasospasm, collateral circulation did not cause ST elevation, but the collateral circulation could not compensate the O2 requirement of the normal right coronary artery area. Therefore, myocardial ischemia occurred and the patient felt chest pain. When the vasospasm disappeared, the collateral also vanished.
In conclusion, when a total vasospasm occurs but ST elevation isn't detected, transient collateral circulation should be considered.



 XML Download
XML Download