

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Most coronary artery anomalies are found incidentally during angiographic evaluation for other cardiac diseases. Coronary artery fistula (CAF) was first described in 1865, and is not an uncommon anomaly.1) Coronary artery aneurysms, defined as coronary arterial dilatation that exceeds the diameter of normal adjacent segments or the diameter of the patient's largest coronary vessel by 150%, are respectively noted in 0.15% to 4.9% of patients undergoing coronary angiography. The most common cause of coronary artery aneurysm in adult is atherosclerosis.
We experienced a female patient who developed double fistulas detected by transthoracic echocardiography (TTE) and confirmed by coronary angiography. To the best of our knowledge, this is the first case report on concurrent, dual fistulas of ascending aorta and coronary artery to pulmonary artery.
Case
A 64-year-old female was admitted with exertional chest tightness and shortness of breath for several weeks. The chest tightness radiated to the left scapular area occasionally, and lasted more than half an hour. The patient had history of hypertension for 10 years. There was no family history of aortic, collagen, vascular or congenital heart disease.
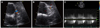
Her vital signs were as follows: blood pressure of 140/90 mmHg, pulse of 70 beats/min, respiration of 20 breaths/min, and body temperature of 36.5℃. On examination, cardiac auscultation revealed 2 to 4 grade diastolic murmurs and her electrocardiography demonstrated no apparent ST segment and T wave abnormalities. Blood chemistries, including coagulation studies and complete blood cell count, as well as cardiac enzymes and lipid profiles, were within the normal limits. Her heart size was normal on chest radiograph. TTE Doppler revealed two focal diastolic flows within the pulmonary trunk (Fig. 1A), and a dilated left coronary artery (Fig. 1B) associated with continuous turbulent systolic and diastolic flow patterns (Fig. 1C).
The size of left ventricle was normal with an ejection fraction of 64% and there were no abnormalities in the regional wall motion, cardiac valves. Exercise Treadmill test showed 10 MET positive finding (2 mm ST depression in V5, V6).
Coronary angiography demonstrated no significant narrowing of three major coronary arteries (Fig. 2). However, two large fistulas with aneurysm were noted incidentally. One fistula originated from the ascending aorta (Fig. 2B and C), and another from the proximal portion of the left anterior descending coronary artery (Fig. 2D and E) were detected. Both fistulas drained into the pulmonary artery (Fig. 2B-E). Multi-detector-row computed tomography was performed in order to further evaluate the fistulas associated with aneurysm, which showed that the fistulas were comprised of two source vessels and a single draining vessel (Fig. 3). There was separate ostium of the left main coronary artery and fistula tract (Fig. 3A), which was also confirmed by coronary CT angiography (Fig. 3B, C and D).
Despite medical treatment, her chest discomfort and exertional dyspnea did not improved. We therefore recommended fistula ligation operation. She was transferred to another hospital where she underwent ligation operation. She was asymptomatic following successful ligation of double fistulas.
Discussion
CAF is a congenital abnormality with an estimated frequency of 0.27% to 0.4% of all congenital cardiac lesions,1)2) and usually discovered incidentally at coronary angiography. In addition, CAF can be diagnosed during evaluation of continuous murmur at the precordium, and rarely found during investigation for the etiology of bacterial endocarditis.3)4) The fistula may be single or multiple, isolated or associated with accompanying congenital defects. The hemodynamic effect of CAF depends on the site of drainage and resistance within the fistula.
The most frequent complaints of patients with CAF are angina pectoris, atypical chest pain and lethargy. The pathophysiologic mechanisms of the symptoms are volume overload as a result of the shunt, coronary steal that causes decreased myocardial oxygen supply and lack of capillary formation.5) TTE is an important non-invasive tool for identifying the anomalous origin of coronary arteries, and continuous turbulent systolic and diastolic flow pattern characterizes the shunt entry site.6)7) However, coronary angiography still remains the gold standard for diagnosing coronary anomalies. Selective coronary angiography can be used to reliably identify the size and anatomic features of the fistulous tract, which can be diagnostic and therapeutic.8)
Current treatment options include careful observation, surgical ligation with or without cardiopulmonary bypass, ligation with bypass of the involved coronary artery, and transcatheter embolization. Treatment for asymptomatic fistulas without significant shunting remains controversial.9)10) Small fistulas are usually asymptomatic and managed conservatively. They generally run a benign course and may close spontaneously. Surgical ligation of fistula is limited to larger symptomatic fistula with large branch vessels that may be compromised by occlusion devices. Surgical correction may also be used for coronary fistula with multiple communications. There is general agreement that symptomatic patients, such as our patient, should be treated, and it is well accepted that all symptomatic patients should be treated with surgical ligation or closure. The same applies to those who experience complications.
This is the first report of dual fistulas associated with a large aneurysm originating from the ascending aorta and proximal left anterior descending coronary artery, which were connected to pulmonary trunk. The patient was successfully treated with fistula ligation operation. Because the patient was transferred to a surgical hospital, we were only able to follow up by telephone. She experienced no major cardiac events over one year of follow up.
To investigate chest pain and dyspnea, early evaluation with TTE is useful and remains very important to predict and diagnose the exact disease cause.


 XML Download
XML Download