

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Metabolic syndrome (MS), that is the clustering of abnormalities in glucose metabolism, lipid metabolism, and blood pressure (BP),1) and is associated with an increased prevalence of subclinical damage in a variety of organs. MS increases the risk for the target organ damage in hypertensive (HTN) patients2) and the development of type 2 diabetes mellitus.3)
Hyperuricemia mediates the development of end-organ damage such as increased carotid intimamedia thickness,4) and it is regarded as a cardiovascular risk factor and a determinant of MS,5) although the other studies have concluded that an association between serum uric acid and cardiovascular disease merely reflects the link between serum uric acid and other risk factors.6)
Adiponectin is known to have anti-inflammatory and anti-atherogenic activities7) and adiponectin levels significantly correlated with various indices (including serum uric acid) of MS.8) Circulating levels of retinol-binding protein-4 (RBP4) are elevated in humans with insulin resistance, which is a hallmark of MS. It can also predict early stages in the development of insulin resistance, a major cause of type 2 diabetes as well as cardiovascular disease.9) Impairment of nitric oxide (NO) release is associated with endothelial dysfunction.10)
In this study, we screened the metabolic parameters, renal involvement, uric acid, adiponectin, RBP4, NO and insulin in HTN patients with or without MS. We investigated the relationship between the plasma levels of adiponectin and RBP4 with the other variables of MS in the HTN with MS group. Finally, we also clarified the association between the two types of adipokines (adiponectin, RBP4) and uric acid, which are the known markers of endothelial dysfunction and cardiovascular damage in MS, in the HTN with MS group.
Subjects and Methods
Patients
In total, seventy consecutive patients diagnosed with essential hypertension were enrolled from the outpatient clinic at Bucheon St. Mary's Hospital, Bucheon, South Korea. Hypertension was defined as official systolic BP ≥140 mmHg or diastolic BP ≥90 mmHg. These patients had no history of anti-hypertensive and anti-diabetic treatment and they had not taken lipid lowering agents within the last 6 months. The main exclusion criteria were: the presence of clinical or laboratory evidence of congestive heart failure, atrial fibrillation, previous stroke, significant valvular heart disease, previous myocardial infarction, history of coronary bypass, secondary cause of hypertension, and neoplastic disease. The patients informed consent had been obtained during the initial visit.
The patients were categorized into two groups: HTN without MS group and HTN with MS group. The study protocol was approved by the Ethics Committee of Bucheon St. Mary's Hospital.
Definition of metabolic syndrome
MS was diagnosed when two or more of the following criteria were present in the HTN patients: abdominal obesity (waist circumference >90 cm and >80 cm in women),11) hypertriglyceridemia (>150 mg/dL), reduced high density lipoprotein-cholesterol (HDL-C) (<40 mg/dL in men and <50 mg/dL in women), high fasting blood glucose (≥100 mg/dL).1)
Official blood pressure measurement
BP was measured by nurses during two different visits to the outpatient clinic by using a mercury sphygmomanometer. At each visit, three measurements were taken at 1-minute intervals after the subject had rested for 5 minutes in the sitting position, and the average of the measurements was considered.
Laboratory methods
Blood samples were obtained from the subjects by venipu-ncture and were placed into ethylenediaminetetraacetic acid-containing tubes, the samples were centrifuged to obtain serum; the serum was stored at -70℃. Serum adiponectin levels were determined using a commercially available enzyme-linked immunosorbent assay (ELISA) kit (R&D Systems, Inc., Minneapolis, MN, USA) with a detection limit of 0.1 ng/mL. Serum RBP4 concentration was measured by a commercially available ELISA according to the manufacturer's instructions (AdipoGen Inc., Seoul, Korea). NO levels were measured us-ing a commercial kit supplied by BioAssay Systems (Hayward, CA, USA), which uses metallic cadmium beads to convert nitrates into nitrites. The quantitative insulin sensitivity check index (QUICKI) of insulin sensitivity was calculated from the fasting insulin and fasting glucose values: QUICKI=1/{log (fasting insulin)+log (fasting glucose)} as described by Katz et al.12)
Statistics
The results are expressed as means±standard deviation. Comparisons of the serum markers between the HTN with MS and the HTN without MS groups were analyzed by using the independent t-test. Nonparametric test was also performed using Mann-Whitney test. Correlations between the levels of adiponectin, RBP4, NO and uric acid were also analyzed using the Pearson correlation test. Several multiple linear regression models were also performed by using plasma adiponectin, RBP4 or NO as the dependent variable and using age, body mass index (BMI), creatinine, total cholesterol, QUICKI, and uric acid level as independent variables in the HTN with MS group. All statistical calculations were performed using a commercially available statistical package (SAS, version 8.0, NC). A value of p<0.05 was considered statistically significant.
Results
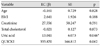
Of the seventy consecutive HTN patients, 26 patients were categorized into HTN with MS group. Considering for age and sex, 12 patients were selected from the remaining 44 patients and they were categorized into HTN without MS group. Only BMI and waist circumference were significantly higher in the HTN with MS group. Serum adiponectin (HTN without MS : HTN with MS=8.57±6.58 : 4.53±4.31, p=0.030) and NO (HTN without MS : HTN with MS=61.2±36.0 : 27.5±22.5, p=0.003) concentrations were lower in the HTN with MS group. Serum levels of RBP4 were elevated in the HTN with MS group, although this was not statistically significant (HTN without MS : HTN with MS=21.3±12.6 : 38.4±29.7, p=0.106). Serum levels of uric acid were higher in both the patient groups (HTN without MS : HTN with MS=4.13±1.26 : 5.03±1.19, p=0.040). Triglyceride levels were elevated and HDL-C levels were reduced in the HTN with MS group (Table 1).
Relationship between classical and novel biomarkers in hypertensive patients with or without metabolic syndrome
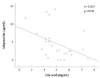
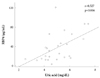
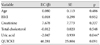
Correlation between two adipokines, uric acid and NO are summarized in Table 2. In the HTN with MS group, serum adiponectin levels were negatively correlated with uric acid (r=-0.413, p=0.036) (Fig. 1) and insulin levels (r=-0.453, p=0.026) and positively with QUICKI (r=0.442, p=0.031). RBP4 levels showed positive correlation with uric acid (r=0.527, p=0.006) (Fig. 2), but serum NO levels did not correlate positively with uric acid, insulin or QUICKI. These correlations were not observed in the HTN without MS group. Multiple linear regression analysis with serum adiponectin and RBP4 levels as the dependent variables revealed that only uric acid correlated independently with serum RBP4 and adiponectin level (Table 3 and 4).
Discussion
We have presented a correlation between the two types of adipokines (adiponectin and RBP4) and uric acid in the HTN with MS group. RBP4 had a positive correlation with uric acid, while adiponectin had an inverse correlation with uric acid. In addition, we also demonstrated that the HTN with MS group had significantly higher values of serum uric acid and lower serum adiponectin and NO levels than the HTN without MS group. The strength of this study was that the subjects were initially diagnosed as HTN had not taken any medications; thus there were no confounding factors such as anti-hypertensive, anti-diabetic and lipid-lowering agents which are known to affect cytokine levels. Secondly, we used multiple linear regression analysis to confirm the association between the two adipokines (adiponectin or RBP4), NO and uric acid, which are the known risk factors of MS and cardiovascular events in HTN accompanying MS.
Our study also showed that the levels of serum uric acid were elevated in the HTN with MS group. Hyperuricemia is related to an increased incidence of high BMI, high BP, high triglycerides and a 10-year probability of coronary heart disease.6)12) It is also associated with insulin resistance and its mechanism is a decreased renal excretion of uric acid.13)14)
Increased serum RBP4 levels were known to contribute to impaired insulin-stimulated glucose uptake in muscle and elevated hepatic glucose production, both of which are characteristic of type 2 diabetes.9) RBP4 level is currently known to be independently associated with uric acid level in patients with type 2 diabetes mellitus.15) Our data showed that serum RBP4 levels were elevated in the HTN with MS group, but was not significantly different than in the HTN without MS group (p=0.106). However, RBP4 was strongly correlated with uric acid which was a cardiovascular risk factor and a determinant of MS.6) The levels of two types of adipokines (adiponectin and RBP4) showed a significant relationship with uric acid in the HTN with MS group and it was stronger between RBP4 and uric acid. Only RBP4 levels showed a independent relationship with uric acid after multivariate regression analysis when considering for age, BMI, creatinine, total cholesterol and QUICKI. Elevated plasma levels of RBP4 are known to be related with cerebrovascular disease and metabolic complication.16)
In our study, serum adiponectin levels were decreased in the HTN with MS group as compared to the HTN without MS group. Adiponectin levels also correlated with uric acid, but this relationship was weaker than the relationship between RBP4 and uric acid. In contrast to the other adipocyte-derived proteins, adiponectin has anti-inflammatory and anti-atherogenic activities. Low levels of adiponectin are considered as a hallmark of MS and increases the risk of insulin resistance, visceral adipocity and related MS.17) The plasma levels of NO were significantly different between the two groups. But NO failed to exhibit a relationship with the other clinical or biochemical markers of hypertension with MS. It may be due to its labile character and a relatively small number of patients in this study.
The limitations of our study are a cross-sectional design and small sample size. Large, prospective, placebo-controlled intervention trials are needed to document whether changing the levels of the two types of adipokines (adiponectin and RBP4) or uric acid by pharmacological treatment might lead to a reduced risk for cardiovascular event.
In conclusion, plasma levels of the two types of adipokines (adiponectin and RBP4) and uric acid showed a correlation in the HTN with a complication of MS group. This result can add further evidence of RBP4 as a marker of metabolic complication in addition to adiponectin, especially in the HTN patients.


 XML Download
XML Download