

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Coronary artery disease (CAD) is one of the most important causes of left ventricular systolic dysfunction (LVSD) and it is found in approximately 68% of patients with LVSD.1) Because left ventricular (LV) function and prognosis can be improved with successful revascularization, differentiation of significant CAD from other non-ischemic etiologies is important in managing these patients. However, in advanced heart failure, it is sometimes difficult to delineate the underlying etiology with echocardiography, because of the features of dilated cardiomyopathy. Patients with dilated cardiomyopathy may present with chest pain or ECG change suggestive of CAD, whereas some patients with CAD and heart failure present without history of angina or electrocardiography (ECG) evidence of myocardial ischemia/infaction (Fig. 1). Conventional coronary angiography is the gold standard method for the diagnosis of CAD. However, it is invasive and associated with nephrotoxicity and other risks. Some patients strongly refuse to undergo invasive coronary angiography. This has led to the development of non-invasive imaging for the diagnosis of CAD, which often involves expensive equipment, radiation exposure, needs medication and contrast administration.2) Carotid intima-media thickness (IMT) is efficient, relatively inexpensive, highly reproducible and does not expose patients to contrast dye and radiation. In addition, carotid IMT is a well established surrogate marker of atherosclerosis and is associated with cardiovascular events and asymptomatic myocardial ischemia.3) Recently, some reports discussed the differentiation of ischemic cardiomyopathy from dilated cardiomyopathy using carotid ultrasonography.4)5) As such, the aim of this study was to explore the predictive value of carotid IMT and plaque for the diagnosis of CAD in severe LVSD patients.
Subjects and Methods
Study population
Between August 2005 and May 2009, 181 newly diagnosed heart failure patients were admitted with LV dilatation {left ventricular end-diastolic dimension (LVEDd) >55 mm} and severe LVSD {left ventricular ejection fraction (LVEF) ≤30% with modified Simpson's method}. We excluded 70 patients with previous history of myocardial infaction (MI), percutaneous coronary intervention (PCI), coronary artery bypass graft (CABG), acute coronary syndrome (ACS) and elevated cardiac enzyme on admission. In addition, we also excluded 38 patients who did not undergo diagnostic work up for coronary anatomy. Seventy-three (n=73) patients underwent coronary arteriography, conventional coronary angiography (64 patients) and CT coronary angiography (9 patients) were included in this study. Decision to perform diagnostic work up for coronary anatomy was at the duty physicians' discretion, according to the patients' clinical features at presentation, including visible Q wave or poor R wave progression on ECG, presence of cardiovascular risk factors and associated chest pain. We classified patients into two groups: the CAD group and the non-CAD group, according to coronary angiographic findings.
Two dimensional echocardiography
Two dimensional images were obtained using standard views in the left lateral decubitus position. LV dimensions were obtained in the standard views. LV end systole and end diastolic volumes were calculated by using the modified Simpson's method, and ejection fraction was calculated from the LV end systole and end diastolic volumes.
Carotid intima-media thickness and plaque definition
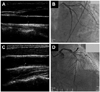
Carotid ultrasound examinations were conducted using commercially available linear array transducer (8.0 MHz linear probe, Acuson sequoia C 512, Siemens, automated measurement). Experienced sonographer obtained images of the far wall of both common carotid artery (CCA) and carotid bulbs according to the Mannheim common carotid IMT consensus. Plaque was defined as a focal structure encroaching into the arterial lumen of at least 0.5 mm or 50% of the surrounding IMT value, or demonstrated a thickness greater than 1.5 mm as measured from the media-adventitia interface to the intima-lumen interface.6)
Each CCA segment was measured and these measurements on both sides were averaged to obtain mean CCA IMT. Thickness greater than 0.9 mm was regarded as increased CCA IMT. We also considered the presence of plaque on either side as positive finding.
Coronary angiography and assessment of coronary artery disease severity
Coronary angiography was performed via the femoral or radial artery using standard technique, and CT coronary angiography was obtained using 64 channel multi detector CT scanner (Lightspeed VCT XT, GE Healthcare, USA). CAD was defined as greater than 70% stenosis in a major epicardial coronary artery. We used the Duke Myocardial Jeopardy Score to evaluate the severity of CAD, categorized as mild (jeopardy score 2-4 points), moderate (6-8 points), severe (10-12 points). In this jeopardy scoring system, the coronary tree is divided into 6 segments: the left anterior descending artery (LAD), diagonal branches, septal perforating branches, circumflex coronary artery, obtuse marginal branches, and the posterior descending coronary artery. Segments distal to stenoses greater than 70% are considered to be 'at risk'. Each such segment is assigned 2 points. The maximum possible number of points is 12.7) For example, significant proximal LAD stenosis makes 6 jeopardy score points (septal perforator: 2 points, diagonal branch: 2 points and 2 points for LAD). Single vessel disease, for example due to right coronary artery (RCA) stenosis, will be awarded 2 jeopardy score points.
Statistical analysis
Data are expressed as mean±SD and frequencies are expressed as percentages. The differences between measurements were tested using t-test for continuous variables and Chi-square test for categorical variables. A probability value of p<0.05 was considered statistically significant. Multivariate logistic regression analysis was performed to determine the independent predictor for CAD. Data were analyzed by using Statview for Windows, version 5.0 (SAS Institute, Inc., Cary, NC, USA), and MedCalc, version 7.0 (MedCalc Software, Mariakerke, Belgium).
Results
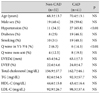
Among the study cohort of 73 patients, there was no significant stenosis in 32 patients (jeopardy score= 0, Non-CAD group), whereas 41 patients experienced significant stenosis (jeopardy score ≥2, CAD group). Three patients were awarded 2 points on the jeopardy score, because all of whom experienced significant stenosis in the RCA. Baseline characteristics of the two groups are summarized in Table 1. There were no significant differences in age (68.3±13.7 years vs. 70.4±13.1 years), male sex (40.4% vs. 59.6%), diabetes (25% vs. 46.3%), smoking (31% vs. 48.3%), LVEDd (63.4±6.2 mm vs. 63.1±7.5 mm), LVEF (22.6±4.6% vs. 24.0±4.7%). The prevalence of hypertension (34.3% vs. 65.8%, p<0.01) and Q wave in V1-4 (6.3% vs. 14.3%, p<0.01) was significantly higher in the CAD group.
Carotid ultrasonographic findings and coronary artery disease
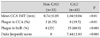
Mean CCA IMT was significantly higher in the CAD group than in the non-CAD group (0.74±0.05 mm vs. 1.04±0.04 mm, p<0.01) (Figs. 1 and 2A). Comparing patients with jeopardy score between 2 and 4 points (the mild group), and patients with jeopardy score between 10 and 12 points (the severe group), the latter demonstrated more increased CCA IMT (0.86±0.15 mm vs. 1.04±0.24 mm, p<0.05) (Fig. 2B). Plaque in CCA (6.25% vs. 19.5%, p<0.01), and plaque in bulb (25.0% vs. 60.9%, p<0.001) were more frequently found in the CAD group (Table 2).
Diagnostic accuracy of carotid ultrasonography for the prediction of coronary artery disease
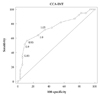
Receiver-operating characteristic curves constructed for different values of mean CCA IMT versus CAD demonstrated the optimal mean CCA IMT cut off value for ischemic etiology (Fig. 3). The area under curve was 0.741 and a cut off value of CCA IMT at 0.9 mm had sensitivity and specificity of respectively 56.1% and 88.2% in detecting CAD and that of a cut off value of 1.0 mm was respectively 35.9% and 94.1% (Fig. 3). The sensitivity and specificity of plaque in CCA in detecting CAD were respectively 19.5% and 93.7% and that for plaque in bulb was respectively 61% and 75% (Table 3).
Predictive factors for coronary artery disease
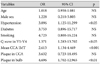
Multivariate logistic regression analysis showed that hypertension {odds ratio (OR) 3.0, 95% confidence interval (CI) 1.12-11.29, p<0.05}, mean CCA IMT (OR 2.61, 95% CI 1.134-4.469, p<0.01) and plaque in bulb (OR 4.69, 95% CI 1.702-12.965, p<0.01) were significant predictors for CAD (Table 4).
Subgroup analysis for low probable group
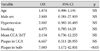
Among 29 patients classified with low probability for CAD (no history of diabetes mellitus, no Q wave in ECG), 8 patients (27.6%) were shown to have significant CAD (jeopardy score 4 in 3, 8 in 2 and 10 in 3 patients). The presence of plaque in bulb was a significant predictor for CAD (OR 7.08, 95% CI 1.17-42.8, p<0.05) in patients classified as low probability (Table 5).
Discussion
In daily medical practice, it remains a challenge to distinguish between ischemic and non-ischemic cardiomyopathy. Ischemic etiology has been shown to be independently associated with worse long-term outcome in patients with LVSD.8) The etiology of cardiomyopathy also influences the decision to pursue revascularization and the choice of pharmacologic intervention.9)
Dilated cardiomyopathy, defined as LVSD with chamber dilatation, represents a final common pathway for many pathologic processes. No clear etiology can be identified in a substantial proportion of cases. For example, 8% of CAD was found in transplantation candidates diagnosed with idiopathic dilated cardiomyopathy.10) In patients with definite history of MI, PCI, CABG, ACS and elevated cardiac marker, there was no uncertainty on the ischemic etiology of cardiomyopathy. We did not hesitate to perform coronary angiography, unless patients refuse invasive procedure. However, in certain patients, determination of etiology may be difficult because patients with heart failure without CAD may present with typical angina or regional wall motion abnormalities on echocardiography, whereas patients with severe CAD may present without symptom of angina or history of myocardial ischemia/infaction. Carotid IMT is a well-established surrogate marker of coronary atherosclerosis,11)12) and is associated with cardiovascular events.13) It is efficient, relatively inexpensive and highly reproducible and does not expose patients to contrast dye or radiation. Previous studies demonstrated the relationship between carotid IMT and the extent and severity of coronary stenosis.14-19) Therefore, it can be postulated that carotid IMT and plaque provide diagnostic clue for ischemic etiology in severe LVSD patients. Atherosclerosis is a systemic disease and, as such, increasing carotid IMT and plaque are correlated with CAD. However, this association remains debatable.20) Our study demonstrated that mean CCA IMT is higher in the CAD group (Fig. 2) and mean CCA IMT is increasing according to coronary jeopardy score, which is a simple method for estimating the amount of myocardium at risk on the basis of coronary artery stenosis. Even after having excluded patients with known ischemic history, significant CAD was found to exist in 41 patients (56.1%) in our study population. Among 29 patients classified with low probability of developing CAD, CAD was found to exist in 8 patients (27.6%) and plaque in bulb remained statistically significant predictor for CAD. We therefore conclude that detection of CAD of unknown etiology in severe LVSD patients is important, because they need revascularization that can improve prognosis. In addition, our study demonstrated showed good specificity of mean CCA IMT (93.7%) (Fig. 3) and the presence of plaque in bulb also exhibited relatively good specificity (75%) and positive predictive value (80%) for the diagnosis of CAD (Table 3). Therefore, we weighted on mean CCA IMT or the presence of plaque can be used as tools to support the presence of ischemic etiology in severe LVSD patients and normal CCA IMT in the absence of plaque support the non-ischemic etiology of severe LVSD patients. In practice, if severe LVSD patients have no history of ischemia with normal IMT and without plaque in bulb, we can initially classify them as non-ischemic LVSD. On the contrary, increased IMT with plaque in bulb in patients are indications to perform coronary angiography.
Based on our findings, mean CCA IMT and plaque in bulb can be useful tools for the prediction of CAD in severe LVSD patients with unknown etiology.
Limitations
This study is limited by the small sample size and its retrospective nature. In addition, there might have been inherent selection bias because we did not include all patients with severe LVSD. It may not be clinically justified to perform coronary angiography in all patients due to the low probability of atherosclerosis, particularly in young patients.
Conclusion
Mean CCA IMT was higher with CAD group in severe LVSD patients. And mean CCA IMT and plaque in bulb were good predictors for CAD. CCA IMT and plaque in bulb showed good specificity and positive predictive value for CAD. In patients with severe LVSD, mean CCA IMT and plaque in bulb can be useful additional tools for the prediction and/or exclusion for CAD.


 XML Download
XML Download