

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Mirror image dextrocardia was first noted in the 1920s and it may be present in about one in 130,000 people. Although dextrocardia occurs rarely, the incidence of coronary artery disease is similar to the general population.1)2) Successful coronary angiography and angioplasty via the femoral artery have previously been performed in patients with dextrocardia.3)4) But, there has been no report on transradial coronary angiography in a patient with dextrocardia in Korea. We report a case of successful transradial coronary angiography in a patient with right sided heart.
Case
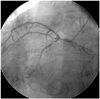
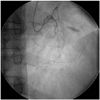
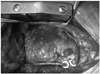
A 54-year-old man with dextrocardia presented with severe exertional chest pain. He had been managed for hypertension, hypercholesterolemia, and diabetes mellitus. Chest X-ray showed a rightwardly displaced cardiac apex. Exercise testing using the Bruce protocol reproduced his symptoms within the second stage of the test. Because of his right handedness, coronary angiography was performed from the left radial artery. Selective coronary angiograms were obtained using counter-directional torquing of Judkins Left-4 and Amplatz Left-2 catheters and mirror-image angiographic angles. The left main coronary artery was 60% stenosed in the distal bifurcation, with significant narrowing of both proximal left anterior descending and left circumflex arteries (Fig. 1). The non-dominant right coronary artery was diffusely occluded at its mid segment (Fig. 2). He received bypass surgery due to multivessel disease with left main stem involvement. Instead of the left internal mammary artery, the right internal mammary artery was harvested for his right sided heart (Fig. 3).
Discussion
Dextrocardia is a rare cardiac condition in which the incidence of coronary artery disease is presumably similar to the general population.1)2) Since the first diagnostic cardiac catheterization in a patient with dextrocardia in 1973,2) few have reported transfemoral catheterization procedures.3)4)
The most important modifications in performing coronary angiogram in patients with dextrocardia are opposite-direction catheter rotations and mirror-image angiographic angles, i.e., anticlockwise rotation in the ascending aorta for the right coronary artery and reversing the required right anterior oblique/left anterior oblique angles but keeping the cranial/caudal tilts the same.3)4) Other angiographers used a double-inversion technique, which normalizes all angiographic pictures to the standard conventional pictures as seen in a normally located heart.5) In our case, we performed coronary angiography with a novel transfemoral approach, the counter-directional torquing of the catheter, as well as right-left mirror-image inversion angiographic views.3)4) We did not do further image reversal to employ traditional views.
Nowadays, transradial coronary angiography is gaining popularity because it can make patients comfortable, reduce vascular complications, and allows earlier ambulation than the transfemoral technique.6) However, there has been no report on transradial coronary angiography in these patients in Korea. Although transradial angiography is probably more difficult than transfemoral angiography due to potential subclavian or innominate arterial tortuosity and/or angulation, we selected transradial coronary angiography. Moreover, we chose a left approach because of his right handedness. We assumed that the left transradial approach might be similar to right transradial angiography in patients with normal heart position, except for the unfamiliarity for angiographer.
There has been no consensus in selecting imaging catheters. Moreyra et al.3) reported that regular coronary catheters (Judkins) are difficult to use because of the reversed position of the coronary ostia, and recommended nontraditional catheters with wider curves and longer tips. Otherwise, both the left and right coronaries were successfully cannulated with Judkins catheters in other reports.4) In our case, left coronaries were easily engaged with a Judkins Left-4 catheter, but we used an Amplatz Left-2 catheter for the right coronary artery because of its tortuosity and leftwardly displaced origin. The use of opposite-directional torquing of these catheters in mirror-image angiographic angles allowed uncomplicated left transradial angiography in a patient with right sided heart, dextrocardia.
In summary, our report demonstrates the feasibility of left transradial angiography in the rare patient with dextrocardia, suggesting its potential as a simple approach to the right sided heart.
 XML Download
XML Download