

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Left ventricular hypertrophy (LVH) and increased left ventricular mass index (LVMI) are well known cardiovascular prognostic predictors.1)2) In patients with stable coronary heart disease, increased LVMI is independently associated with all-cause mortality and sudden or arrhythmic death, even in subjects with normal ejection fraction.3) Many factors such as blood pressure, circulatory volume load as well as age, body size and sex can influence left ventricular (LV) mass.4)5) Currently, osteoporosis has been suggested as another risk factor associated with cardiovascular disease.6)7) In addition, low bone mineral density (BMD) in postmenopausal women is associated with increase in cardiovascular mortality.8) In the recent Framingham study, low bone mass showed correlation with coronary artery disease in women.9) According to studies in primary hyperparathyroidism, increased parathyroid hormone and serum calcium can affect cardiomyocytes, vascular endothelial cells and vascular smooth muscle cells.10) This could lead to hypertrophy of cardiomyocytes and vascular endothelial cell dysfunction, finally resulting in cardiac diastolic dysfunction and cardiac hypertrophy. Moreover, the causal relationship between low BMD and LVMI in postmenopausal women could be explained by hormonal changes, for example, decreased osteoprotegrin (OPG) levels in this population.11) Although a pathophysiological association between calcium metabolism and LVH has been suggested, few epidemiologic studies have been performed. The objective of this study was to investigate the association between BMD and LVMI in a general population.
Subjects and Methods
Study population
A cross sectional analysis was performed on a general population who lived in rural area, Korea from 2004 to 2005. A total of 543 subjects were sampled from the general population and informed consents were obtained from 502 subjects at study entry. Subjects were required to answer a questionnaire which included basic demographic, social economic information and past medical history. Lifestyle parameters including smoking, drinking, daily physical activity and dietary patterns were reviewed. Among these subjects, an echocardiography, carotid intima-media thickness (IMT), brachial-ankle pulse wave velocity (baPWV) and BMD were performed in 468 subjects. A complete physical examination including height, weight, waist circumference, heart rate and blood pressure was done and blood chemistry including fasting blood glucose (FBG) and lipid profile were analyzed. In total, 42 subjects were excluded due to incomplete data (n=34) and pre-existing cardiovascular disease (n=8). Subjects with hypertension or under treatment with antihypertensive medications (112 subjects, male 49%) and diabetes (34 subjects, male 41%) were included in the analysis. Finally, 460 subjects were included in the analysis.
Echocardiography
Two-dimensional and guided M-mode echocardiograms were performed on each subject by a single cardiologist using a commercially available machine (HP SONOS 2500; Hewlett Packard, USA) with a 2.5/2.0 MHz transducer. Measurements for M-mode guided calculations of LV mass were taken at or just below the tip of the mitral valve with a paper speed of 50 mm/sec. The LV internal end-diastolic dimension, end-systolic dimension (LVID), inter ventricular septal thickness (IVST) and posterior wall thickness (PWT) were measured on the leading edge, according to the guidelines of the American Society of Echocardiography. LV mass was calculated using the following equation: LV mass={1.04×(IVSTd+LVDd+PWTd)3-LVIDd3}×0.8+0.6.12) LVMI was calculated using the following equation: LVMI=LV mass/height2.7.5)13)
Doppler echocardiographic recordings were performed by pulse-wave Doppler with the sample volume at the tips of the mitral valve in the apical four-chamber view and recorded at a paper speed of 100 mm/sec. Early (E) and late (A) diastolic peak velocities and deceleration time were determined, as previously reported.14)
Bone mineral density
BMD was measured by the Sahara Clinical Bone Sonometer (Hologic Inc., Waltham, MA, USA) which is a radiation-free, waterless, dry system. It consists of two unfocused transducers mounted coaxially on a motorized caliper. One transducer acts as transmitter and the other as receiver. The Sahara device measures both broadband ultrasound attenuation (BUA) and the speed of sound (SOS) at a fixed region of interest in the mid-calcaneus. BUA, expressed in decibel per megahertz (dB/MHz), is the slope of attenuation as a function of frequency as ultrasound waves pass the heel. SOS, expressed in meters per second (m/second), is the transit velocity of a high frequency sound wave through the heel. The results are combined to provide an estimate of heel BMD in units of grams per square centimeter, using the following equation:15)
BMD=0.002592×(BUA+SOS)-3.687 g/cm2
Brachial-ankle pulse wave velocity
BaPWV was measured based on conventional methods with the use of automatic waveform analysis (VP-2000; Colin Medical Technology Co., Komaki, Japan) after resting in the supine position for at least 5 minutes following stabilization of the heart rate.16) baPWV between the bilateral brachial arteries and the ankle was measured by placing both arms and the ankle in a cuff, to which an oscillometric sensor was implanted. The mean of the left and right baPWV was used in the analysis.
Carotid intima-media thickness
The bilateral common carotid arteries (CCAs) were measured using the SA 9900 system (Medison Co. Korea) with a 7.5-MHz linear transducer. Scanning was performed at the far wall of the middle and distal CCAs using a lateral longitudinal projection. The authors decided on the measurement protocol according to previously published epidemiologic studies, and defined IMT at the CCA as the distance between the leading edge of lumen-intima interface and the leading edge of the media-adventitia interface.17)18) Five measurements were made on each side and the average measurement was used as the IMT. To avoid inter-observer variability, all measurements were performed by the same examiner who was unaware of subject characteristics. Intra-observer variability was already evaluated before including the data in this paper. To evaluate intra-observer variability, 20 subjects were randomly sampled and measurements were made twice on each subject. The correlation coefficient at the left bulb, left common carotid, right bulb and right common carotid area was 0.92, 0.90, 0.92 and 0.91, respectively.
Statistical analysis
Sex stratified analyses were conducted due to different characteristics. Independent t-test and chi-square test were performed to compare the general characteristics and clinical results with sex group. Pearson's correlation and stepwise multiple regression analysis were used to identify significant determinants for BMD and LVMI. The criterion for entry into multiple regression analysis was p<0.05 while the removal criterion was p>0.10. A p of less than 0.05 was considered statistically significant. Data were analyzed using Statistical Package for the Social Sciences (SPSS) 16.0 software (SPSS Inc., Chicago, IL, USA).
Results
General characteristics of study subjects
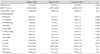
The demographic characteristics of the subjects are summarized in Table 1. The age of the subjects was 59.4±12.4 years. 42.2% (n=194) were male. There was no statistical difference between the gender groups in age, waist circumference, systolic blood pressure (SBP) and diastolic blood pressure, pulse pressure and heart rate. However, significant differences in height, weight and body mass index (BMI) were noted. Although the total cholesterol and low density lipoprotein-cholesterol (LDL-C) levels were higher in female subjects, these profiles were within normal range in both sexes. The proportion of smokers was greater in male than in female subjects.
Clinical characteristics of the subjects
BMD, baPWV, carotid IMT and echocardiographic findings of the subjects are shown in Table 2. BMD, baPWV and carotid IMT of all subjects were within the normal range, 0.47±0.13 g/cm2, 1,510.8±271.0 cm/s and 0.63±0.18 mm, respectively. BMD, baPWV, carotid IMT in male subjects were higher than that of female subjects (BMD; 0.51±0.11 g/cm2 vs. 0.44±0.13 g/cm2, p<0.001, baPWV; 1,539.3±265.0 cm/s vs. 1,490.±273.9 cm/s, p=0.05, carotid IMT; 0.65±0.18 mm vs. 0.61±0.17 mm, p=0.03). The LVMI of study subjects was 47.8±11.4 g/m2.7, and significant difference was not shown between male and female subjects (47.1±10.7 g/m2.7 vs. 48.3±11.8 g/m2.7, p=0.26).
Determinants of bone mineral density
Among the clinical parameters, being female (r=-0.288, p<0.001), age (r=-0.246, p<0.001), waist circumference (r=-0.083, p<0.05), pulse pressure (r=-0.129, p<0.01) and LDL-C (r=-0.187, p<0.001) were negatively correlated with BMD. Current smokers showed negative correlation with BMD (r=-0.140, p<0.001). In male subjects, only age (r=-0.121, p<0.05) showed correlation with BMD, whereas in female subjects, age (r=-0.356, p<0.001), waist circumference (r=-0.103, p<0.05), SBP (r=-0.126, p<0.05), pulse pressure (r=-0.209, p<0.001), FBG (r=-0.115, p<0.05) and LDL-C (r=-0.148, p<0.01) showed negative correlation with the BMD. BMI was positively correlated with BMD (r=0.149, p<0.01). In the stepwise multiple regression analysis, sex (β=-0.312, p<0.001), age (β=-0.182, p<0.001), BMI (β=0.382, p<0.001), waist circumference (β=-0.342, p<0.01) and LDL-C (β=-0.087, p<0.05) were independent determinants of BMD. BMI, waist circumference as well as age were determinants of BMD in the female subjects (Table 3).
The relevance of left ventricular mass index and bone mineral density
Separate analyses were conducted for men and women due to their different general characteristics. BMD correlated with baPWV, carotid IMT and LVMI in female subjects (Table 4) (Fig. 1). Five models were used to estimate the relevance of LVMI and BMD (Table 5 and 6). The first model adjusted for age, current smoking, BMI and SBP (smoking was not adjusted in females due to low prevalence of smokers among female subjects) showed that although BMI and SBP were independent determinants of LVMI in male subjects, BMD was not an independent factor. However, in female subjects, BMD was an independent determinant of LVMI (β=-22.123, p<0.0001). In model 2, additional variables such as abdominal circumference, fasting glucose and lipid profile were included. In model 2, although BMD did not have an effect in males, BMD (β=-18.659, p=0.01) was an independent determinant for LVMI along with BMI and SBP in female subjects. In models 3 and 4, after adjusting the clinical parameters in model 2, the individual effects of arterial stiffness parameters such as baPWV and carotid IMT on LVMI were evaluated. Although baPWV was not related to LVMI, carotid IMT showed an independent effect on LVMI in both male and female subjects (β=10.262, p<0.018, β=21.456, p<0.0001, respectively). Finally, in model 5, the relationship between BMD and LVMI was evaluated, after adjusting not only previous clinical parameters noted above but also baPWV and carotid IMT. BMD did not have an effect in male subjects (β=-1.235, p=0.841). However, it was a negative determinant for LVMI in female subjects, along with BMI and carotid IMT (β=-13.703, p=0.016).
Discussion
The main finding of the study is that BMD is a consistent determinant of LVMI in postmenopausal female subjects. Furthermore, BMD is independent of BMI, blood pressure, chemistry profiles, and the parameters of arterial stiffness such as carotid IMT and baPWV in determining LVMI. This finding suggests that the pathophysiological concept derived from primary hyperparathyroidism can be applied to the relationship between BMD and LVMI in postmenopausal female patients. In primary hyperparathyroidism, increased serum calcium and osteoporosis could lead to hypertrophy of the cardiomyocytes and vascular endothelial cell dysfunction, finally resulting in cardiac diastolic dysfunction and cardiac hypertrophy.10) It is well known that LVMI is determined not only by hemodynamic factors, such as systolic blood pressure and arterial stiffness, but also by non-hemodynamic factors such as obesity. BMD is a non-hemodynamic factor and the interpretation of the relationship with LVMI could be confounded by many factors. For optimal adjustment of hemodynamic factors, we included baPWV and carotid IMT, which are stiffness parameters for peripheral or central arteries, respectively, in the multiple regression model. This was important because arterial stiffness may have clinical relevance in the age (59.4±12.4 years) of this study population.
In this study, BMD as a non-hemodynamic factor that showed correlation with LVMI in female subjects only (Table 4) (Fig. 1). According to the stepwise multiple linear regression analysis compensated with various clinical parameters along with baPWV and carotid IMT, BMD was a consistent and independent determinant for LVMI in female subjects (Table 6). These findings are comparable to that in previous studies, which reported that non-hemodynamic factors were more important in female subjects.19)20) Although more study is needed to clarify the causal relationship between low BMD and LVMI in postmenopausal women, hormonal changes in this population may be a possibility. For example, a change in hormones, including OPG in postmenopausal women, is involved in LV hypertrophy and vascular calcification as well as reduction in bone mass.11)21)22)
The relationship between BMD and baPWV or carotid IMT was also more definite in female subjects (Fig. 1). BMD was a greater determinant in cardiovascular change in female subjects, compared to male subjects. The difference between sexes may be explained by the following clinical characteristics: BMI was higher in female subjects (25.0±3.6 vs. 23.9±2.9, p<0.001), LDL was also higher (107.2±31.8 vs. 91.1±32.3, p<0.001) and BMD was lower compared to male subjects (0.44±0.13 g/cm2 vs. 0.51±0.11 g/cm2, p<0.001). Generally, in subjects of this age group (59.4±12.4 years), BMD is lower in female compared to male subjects, and this could be due to differences in hormonal changes at this age.
According to the findings of our study, low BMD has harmful effects on the vascular structure and/or stiffness. Subsequently, increased arterial stiffness may contribute to LV hypertrophy. But considering that the effects of low BMD on LVH are independent, even after adjusting baPWV and carotid IMT, suggestive that low BMD could have direct influence on LV hypertrophy.
These results attribute to previous reports on the possibility of osteoporosis as a risk factor for cardiovascular disease.6)7) Moreover, osteopenia or osteoporosis and atherosclerotic vascular disease (coronary artery disease, ischemic stroke, or peripheral arterial disease) are common conditions in postmenopausal women.23)24) Osteoporosis and vascular calcification have been largely attributed to the aging process. However, recent studies have shown that arterial calcification is a highly regulated process, with intriguing similarities to bone turnover that may be age-independent.25)26) In a previous study, low BMD was associated with increased risk of ischemic stroke, and was found to be a possible predictor for first stroke among older women.27)28) In another study, osteoporosis was linked to peripheral arterial disease independent of age and gender,29) and low BMD correlated with ankle-brachial indexes.30) In our study, we also found that in postmenopausal women, low BMD contributes to central and peripheral vascular stiffness, which are reflected by carotid IMT and baPWV, respectively. Moreover, we found that decrease in BMD has a weak, but definite contribution to increase in LVMI, leading to LVH even before osteoporosis sets place in postmenopausal women. From the standpoint of clinical relevance, the consistent relationship with relatively low strength between BMD, cardiac and vascular surrogates suggests that more evidence is needed for bone mineral metabolism to be generally accepted as a clinically valuable mechanism for cardiac and vascular health.
This study was a cross sectional analysis and BMD was measured by bone sonometer in the calcaneal bone, not the lumbar spine or femur neck, which limit result interpretation. For a hard endpoint on this subject, a large scale prospective study is warranted. However, this study gives us insights into the relationship between BMD and various cardiovascular parameters in postmenopausal female subjects. We found that BMD serves as a consistent and independent factor in determining LVMI, baPWV and carotid IMT in postmenopausal female subjects.






 XML Download
XML Download