

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
There are many clinical predictors of adverse outcomes after acute myocardial infarction (AMI). Although various kinds of risk scores1)2) and individual risk factors are already in use in clinical practice, many research centers are searching for better predictive tools. Recently, the prognostic value of N-terminal brain natriuretic peptide (NT-proBNP) in acute coronary syndrome (ACS) has been demonstrated in many studies.3)4) In one of the largest NT-proBNP studies on ACS, NT-proBNP had a stronger correlation with mortality than any other markers studied, including cardiac troponin T and C-reactive protein.4)
NT-proBNP is released from myocardial cells in response to volume expansion in heart failure (HF) and is therefore used for early diagnosis of symptomatic or asymptomatic HF.5) In addition, NT-proBNP is released in stressed cardiac walls in ACS before myocardial necrosis, so the measurement of NT-proBNP can provide an early estimate of the risk of ACS.6)7)
However, a diagnostic NT-proBNP cut-off value in ACS has proved difficult to establish as NT-proBNP levels are influenced by various factors including sex, age, renal function, HF severity and obesity. The normal values tend to increase with age and to be higher in women than in men.8) NT-proBNP is cleared by the kidney, so its plasma concentration is elevated in decreased renal function states.9) Furthermore, NT-proBNP levels decrease with higher body mass index (BMI).10)11)
With the lowering effect of obesity on NT-proBNP levels in mind, we investigated the influence of obesity on the prognostic value of NT-proBNP in ACS.
Subjects and Methods
Patient population and study design
This study included the 2,736 patients with AMIs among 12,841 patients registered at the Korean Acute Myocardial Infarction Registry (KAMIR) from January 2005 to September 2008. The KAMIR is a prospective, multi-center, observational registry designed to examine current epidemiology, in-hospital management, and outcome of patients with AMIs in Korea for the commemoration of the 50th anniversary of the Korean Circulation Society.12) To focus on NT-proBNP and obesity in AMI patients, we excluded: patients less than 20 or more than 90 years of age, patients with previous HF, patients with renal insufficiency (elevated serum creatinine level above 2.0 mg/dL) and missing or uncertain data. This left 2,736 patients for final analysis. Major adverse cardiac events (MACE) for one year clinical follow-up were evaluated and defined as the composite of 1) cardiac death, 2) non-fatal myocardial infarction (MI), 3) re-percutaneous coronary intervention, 4) coronary artery bypass graft. We analyzed baseline demographic and clinical characteristics, and related laboratory results including NT-proBNP (pg/mL) which was measured on arrival. In order to investigate the relationship between NT-proBNP and MACE, we defined AMI patients free of MACE as group I and patients who developed MACE as group II. Each group was further divided into men (n=1,972, 70%) and women (n=764, 30%), and were grouped as follows based on BMI (kg/m2) in accordance with the World Health Organization (WHO) BMI cut-off values for overweight and obesity in Asians13): 1) Lean (BMI ≤22.9 kg/m2, 2) Overweight (BMI between 23.0 kg/m2 and 24.9 kg/m2), 3) Obese (BMI ≥25.0 kg/m2).
Statistical analysis
We compared the NT-proBNP levels between patients free of MACE (group I) and patients with MACE (group II) during 1 year of clinical follow-up among the lean, overweight, and obese groups. We used the Statistical Package for the Social Sciences (SPSS) for Windows, version 15.0 (SPSS, Inc., Chicago, IL, USA), for analysis. Continuous variables with normal distributions were expressed as the mean±standard deviation and compared with the Student's t-test. Because NT-proBNP and the logarithm of NT-proBNP were not normally distributed in this study, we used the Mann Whitney U test to compare the means of NT-proBNP between groups I and II. Categorical variables were compared with the chi-square test, where appropriate. Multiple linear regression was used to analyze the strength of association between NT-proBNP and BMI after adjusting for age, sex, and renal function. We compared the means of NT-proBNP among the obesity groups by Kruskal-Wallis test. We finally evaluated the prognostic value of NT-proBNP in each obesity group (lean, overweight, obese) by binary logistic regression.
Results
Baseline clinical characteristics of the study population
Among the 2,736 AMI patients who were followed-up for one year, there were 1,977 male patients (72.4%), 1,703 ST-segment elevation myocardial infarction patients (62.2%) and 258 patients with MACE (9.4%). There were 978 (41.6%) obese AMI patients. Baseline clinical characteristics and laboratory findings of the study population are described in Table 1. Patients in group II were older (p=0.015), more likely to have diabetes mellitus (DM) (p=0.011) and had a higher NT-proBNP level (p<0.001) than patients in group I.
Influencing factors of N-terminal brain natriuretic peptide
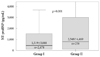
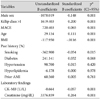
As analyzed by multiple regression (Table 2), significantly influencing factors of NT-proBNP were sex, creatinine level, creatine kinase-MB level, Killip clsass, MACE, age, and BMI. Table 2 demonstrates that NT-proBNP was higher in men, in older patients, with elevated creatinine levels and with lower BMIs (p<0.001 in each case). Fig. 1 shows a box-plot of NT-proBNP and Killip class. NT-proBNP was higher in the Killip class II, III, IV groups than in the Killip class I group (3,353±5,329 pg/mL vs. 1,174±2,240 pg/mL, p<0.001). Fig. 2 shows a box-plot of NT-proBNP in patients with (group II) and without (group I) MACE. NT-proBNP was higher in group II than in group I (2,548±4,469 pg/mL vs. 1,530±3,088 pg/mL, p=0.001).
Obesity and N-terminal brain natriuretic peptide
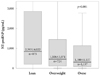
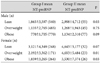
Fig. 3 shows a box-plot of NT-proBNP and three obesity groups as categorized by BMI. The level of NT-proBNP decreased as obesity increased (p=0.001). Table 3 shows the means NT-proBNP levels of each sub-group, divided by sex, obesity degree, and MACE/non-MACE. A notable finding was that the mean NT-proBNP of male obese MACE patients was much lower than the mean NT-proBNP of female lean non-MACE patients (1,134±2,310 vs. 3,121±4,349, p<0.001). Multivariate regression analysis identified BMI as an independent negative correlate of NT-proBNP level (p<0.001) (Table 2).
Prognostic value of N-terminal brain natriuretic peptide related with obesity
For investigation of independent prognostic factors of AMI, we performed multivariate analysis and the results showed that DM, smoking, and NT-proBNP were independent prognostic factors of AMI (Table 4). To focus on the influence of obesity, we evaluated the prognostic value of NT-proBNP in each weight group (lean, overweight, obese) by binary logistic regression (Table 5). NT-proBNP was still an independent prognostic factor of AMI in obese patients (odds ratio=1.009, p=0.01) (Table 5).
Discussion
NT-proBNP is a natriuretic hormone released primarily from the heart ventricles. NT-proBNP is released from myocardial cells in response to volume expansion in HF. Therefore, NT-proBNP has been used for diagnosis of symptomatic or asymptomatic HF.14) However, NT-proBNP is also thought to be released from ischemic myocardial cells due to an unknown mechanism. For this reason, many recent studies have demonstrated the prognostic value of NT-proBNP in ACS patients15)16) Because NT-proBNP levels rise rapidly after the onset of ACS symptoms, NT-proBNP can be used as a good independent prognostic indicator in the early evaluation of ACS patients.17)
However, there are many variables which influence NT-proBNP levels. NT-proBNP is a biologically inert 76 amino acid N-terminal proBNP, produced by cleavage of the prohormone (proBNP) from biologically active 32 amino acid BNP.17) It is cleared by the kidney, with its plasma concentration therefore increased by renal failure.9) The half-life of NT-proBNP is about 120 minutes with normal kidney function.18) We thus excluded renal insufficiency patients (Cr. >2.0 mg/dL) in this study to minimize the influence of kidney function. The plasma concentrations of NT-proBNP are higher in older individuals and in women than in men.8) According to our results, and as expected, NT-proBNP concentrations of women and older patients were significantly higher than those of young and male patients. Another influencing factor is HF. We excluded patients with previous HF history from the study population. The Killip classification categorizes AMI patients based upon the presence or absence of simple physical examination findings that suggest left ventricular (LV) dysfunction (HF).19) Killip class I means no evidence of HF, with increasing Killip class number indicating increasing severity of HF. Our results showed significantly higher NT-proBNP levels with Killip class II-IV (HF) than with Killip class I (non-HF). Finally, another factor strongly influencing NT-proBNP concentration is obesity. Many studies have shown that obese patients tend to have lower plasma NT-proBNP concentrations than nonobese patients.20)21) One study recently announced that BNP levels cannot be used as a marker of LV wall stress in obese individuals.22)
The aim of this study was to examine the influence of obesity on NT-proBNP as a prognostic value in AMI patients of the KAMIR during 12 months of follow-up. We hypothesized that NT-proBNP in obese AMI patients could not be used as a prognostic factor of AMI due to the influence of obesity. Our results demonstrated that obese AMI patients have a lower level of NT-proBNP than lean or overweight AMI patients. The lowest mean NT-proBNP value was seen in male, obese, non-MACE patients (Table 3). Notably, the mean NT-proBNP of male obese MACE patients was markedly lower than the mean NT-proBNP of female lean non-MACE patients. However, NT-proBNP still had an independent prognostic value for AMI among obese patients. This result suggests that obese AMI patients with higher NT-proBNP have worse prognoses.
The mechanism of negative correlation of NT-proBNP and obesity is not yet known. Some authors have suggested that reduced secretion of natriuretic peptides from either diminished myocardial hormone release23) or impaired synthesis24) is the major cause of the inverse relationship between natriuretic peptides and BMI.
There are several limitations to this study. First, our study was a multi-center prospective registry, and it was not a randomized, controlled study. Thus, there was probably a selection bias when enrolling patients into both study groups. Second, we divided our groups according to BMI based on the World Health Organization cut-off values for overweight and obesity in Asians. This will inevitably make it difficult to directly compare our results with those of similar studies of non-Asian patients. Third, the period of our study was relatively short as it was a comparison of MACE during 1 year clinical follow-up. Fourth, we were not able to include the follow-up NT-proBNP or BMI data. Another study demonstrated that early phase NT-proBNP (measured at 2-6 days after AMI) was a better prognostic factor than acute phase NT-proBNP (measured on arrival).25)
In conclusion, NT-proBNP is lower in obese AMI patients than in non-obese AMI patients, but NT-proBNP is still of independent prognostic value for obese AMI patients. Further study will be necessary to investigate the complex relationships between MACE, BMI, sex, and NT-proBNP.




 XML Download
XML Download