

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The autonomic innervation of the heart is rich and asymmetric.1) The postganglionic parasympathetic neurons are primarily located in the fat pads, whereas the postganglionic sympathetic nerves originate from the extracardiac sites, the stellate ganglia, and the sympathetic trunks, and course along the great arteries. Canine hearts have three well-known epicardial fat pads that contain cardiac ganglionated plexi (GP) of the autonomic nervous system. The major GPs are the right pulmonary vein (RPV) fat pad (the so-called sinus nodal fat pad), the inferior vena cava-left atrium (IVC-LA) fat pad [the so-called atrioventricular (AV) nodal fat pad], and the superior vena cava (SVC)-aorta fat pad (the so-called third fat pad), which are referred to as the "head station."2) In the human heart, the existence and location of epicardial fat pads also seem to be similar with those of the canine heart.3)4)
Both vagal and sympathetic stimulation can shorten the atrial effective refractory period (ERP), action potential duration, and re-entrant wavelength. Vagal activation also affects the duration of the refractory period and the heterogeneity of refractoriness. The initiation and maintenance of atrial fibrillation (AF) are highly dependent on these electrophysiologic characteristics; therefore, they could be important in the pathophysiology of AF.
The effects of denervation on ventricular arrhythmia has been evaluated in animal models by several investigators.5) The effects on AF has also been introduced using animal models. AF was not inducible after major epicardial fat pad ablation.2) Fat pad ablation was also achievable by a transvenous approach to suppress AF.6) In humans, GP ablation combined with PV isolation has a reasonable success rate.7-9)
Botulinum toxin (BT) is a neurotoxin produced by Clostridium Botulinum, which functions as zinc-binding metalloendopeptidases. The mechanism of action is blocking of exocytotic release of acetylcholine stored in synaptic vesicles.10) Therefore, BT blocks cholinergic neurotransmission, which is important in postganglionic neurons. Injection of BT into the sinus nodal fat pad blocks bradycardia mediated by parasympathetic activation in the dog heart.11) This study was designed to elucidate the acute effects of blocking the right atrium-pulmonary vein (RA-PV) and left atrium-inferior vena cava (LA-IVC) fat pads on the electrophysiologic characteristics of the atrium and AF inducibility with BT.
Materials and Methods
Surgical preparation
This study protocol was approved by the Seoul National University Hospital Institutional Animal Care and Use Committee. Eight adult male mongrel dogs weighing 15-20 kg were studied. Following standard and approved protocols, all dogs were anesthetized with thiopental (20 mg/kg IV), intubated, and oxygenated followed by gaseous anesthesia (1-2% isofluorane/O2). All measures were taken to ensure that discomfort, distress, pain, and injury were limited to that which was unavoidable. Standard surface ECG leads were monitored continuously throughout the entire study. Intermittent arterial blood gas measurements were obtained and ventilator adjustments were made to correct any metabolic abnormalities. An electrical heating pad was used to maintain body the temperature at 36-37℃.
Vagal stimulation protocol
Bilateral cervical vagal stimulation (VS) was applied using stainless steel electrodes (Model 6491, Unipolar Pediatric Temporary Pacing Lead; Medtronic, Minneapolis, MN, USA) at intensities sufficient to double the sinus cycle length. Typical parameters for the cervical VS trains were a frequency of 20 Hz, a pulse width of 0.2 ms, and a current amplitude of 4-10 V with a Grass stimulator (S-88; Astro-Med, Warwick, MA, USA).
Botulinum toxin injection
A median thoracotomy was performed. After exposure of the posterior side of the heart, BT (50 U/1 mL in each fat pad of six dogs Allergan, Inc., Irvine, CA, USA) or normal saline (NS, 1 mL in each fat pad of two dogs) was injected epicardially to the entire visible areas of the two major epicardial fat pads (RPV and IVC-LA fat pads). The dose of BT used in this study was within the range of the usual clinical dose, therefore the systemic effects were insignificant. The locations of both fat pads are illustrated in a previous report.12) The needle tip was positioned manually at several points on the epicardial surface of the fat pads under direct visual control to ensure optimal injection.
Electrophysiologic study protocol
The study protocol was applied before BT or NS injection and repeated 1, 2, 3, 4, and 5 hours later. Electrocardiographic and atrial electrograms were amplified and filtered from 0.05-500 Hz, and were displayed and recorded on a Prucka Cardiolab EP System (GE Medical Systems, Fairfield, CT, USA). Two epicardial pacing electrodes (Capsure Epi, Medtronic, Minneapolis, MN, USA) were placed at the right atrial free wall. Atrial pacing was performed with twice the current threshold. AV nodal function was evaluated by measuring the ventricular response rate during rapid atrial pacing (RAP) with 50-ms cycle length, mimicking the ventricular response during AF. The sinus and ventricular rate was calculated using the average RR interval of 20 beats. AF inducibility was evaluated with burst pacing using 200 impulses at a 50-ms cycle length, which was performed 4 times in each animal during VS. Spontaneous AF that lasted >30 seconds after the end of the burst stimulation was defined as sustained. The incidence of sustained AF expressed as a percent of the total attempts was defined as AF inducibility.
Results
Effects on the sinus and atrioventricular nodes
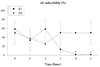
Visually-estimated myocardial contractility was grossly intact during the study. The sinus nodal function was suppressed during VS. VS reduced the sinus rate (57±14% vs. non-VS) before fat pad injection. The effect on sinus rate reduction was decreased gradually to 82±22% five hours after injection of BT (Fig. 1A). However, these changes were not remarkable after injection of NS. The denervation effect of BT on the sinus node was significant 3 hours after BT injection.
The AV nodal function was also suppressed during VS. The ventricular response rate during VS was reduced to 39±22% in comparison to non-VS. This effect was decreased gradually to 66±35% at 5 hours (Fig. 1B). However, the denervation effect of BT on the AV node was not significant. Ventricular response rate patterns were not different statistically between BT and NS.
Effects on atrial fibrillation inducibility
AF inducibility was 58±29% before injection. AF was significantly reduced 3 hours after injection, and AF was not induced at 4 and 5 hours in the BT group (Fig. 2); however, suppression of AF inducibility was not observed in NS group.
Discussion
Major findings
This is the first study to evaluate the effects of GP blocking using BT on AF inducibility in the dog. The VS effects on the sinus node and AF inducibility were significantly eliminated a few hours after BT injection. These findings suggest that short-term denervation of the atria may be achievable by BT in this canine model.
Long-term effects of GP block utilizing radiofrequency ablation on cardiac innervation might be difficult to achieve. It has been demonstrated in an animal model.12) In addition, human GP ablation for the management of patients with AF has been evaluated by several investigators. The effectiveness and outcome of GP ablation as a stand-alone therapy do not seem to be as good as conventional PV isolation procedures.13)14)
However, short-term GP block would be applicable in some clinical field, such as prevention of post-cardiac surgery AF, although its mechanism has not been well-established. For this purpose, a temporary GP block without permanent destruction of GP using BT would be a novel management. To consider human application, the safety of the procedure should be evaluated and how long the denervation effects persist should be determined.
Different vagal effects on the sinus and atrioventricular nodes
The denervation effect of BT on the AV node was not remarkable. One has to keep in mind that we injected BT into only two major epicardial fat pads. The majority of the right vagal fibers innervate the sinus node and they run predominantly through the RPV fat pad (anterior right GP). In contrast, fewer right vagal fibers reach the AV node via IVC-LA fat pad (inferior right GP). There are more GPs (e.g., superior left GP and inferior left GP) innervating the left atria and the AV node although the IVC-LA fat pad would be the major control station of the AV node. Therefore effective denervation of the AV node might be difficult to achieve by blocking only two fat pads. Such an explanation needs experimental testing by all GPs plus the third fat pad block.
Study limitations
We did not block the third fat pad as well as the left-side GPs in the present study, as described previously. However, total denervation would not be achievable even with ablation of all these GPs, although the completeness of denervation would be higher. This is because efferent fibers bypassing the GPs in dogs have been identified.2) Therefore a 100% denervation might be impossible in any case.
We did not decentralize the cervical vagal trunks, so we cannot rule out the effect of afferent nerve activation. We did not use sympathetic system blockade, such as beta-blocker or sympathetic ganglia destruction. Thus, sympathetic activation during the procedures might have affected the results of the present study. However, we successfully kept all vital signs stable in the animals during the experimental procedures. Therefore, the variation of the sympathetic tone might be minimal.
We did not measure the atrial ERP. Thus, we do not know whether a BT injection affected that ERP could be associated with AF vulnerability.

 XML Download
XML Download