

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Marfan syndrome is a connective tissue disorder resulting from a fibrillin-1 gene mutation. An abnormality in the formation and integrity of elastic fibers in Marfan syndrome causes weakening of the aorta, leading to dilatation and dissection. Aortic root dilation is the most common cause of morbidity and mortality. If the aortic root dilates to 5 cm or more, then prophylactic surgery should be considered. There are three techniques in the Bentall procedure including the classic technique, the button technique, and the Cabrol procedure that are commonly used techniques for re-implantation of coronary arteries after repair of the ascending aorta.1-5) The Cabrol technique includes replacement of the ascending aorta and aortic valve using a composite graft. Then, a second Dacron tube graft (approximately 60-80 mm in length) is used with one end fashioned in an end-to-side anastomosis with the ascending aortic graft, and the other as an end-to-end anastomosis with the native coronary ostia.6) Though there have been several reports about percutaneous intervention of the chronic stenotic Cabrol graft-coronary ostial anastomotic lesions,7-10) the case with acute graft thrombosis has not been reported. Koh et al.11) reported 2 cases (25%) of mortality when they performed a modified Bentall operation due to left ventricular failure, arrhythmia and bleeding.
Here we report the first case of acute ST segment elevation myocardial infarction caused by thrombosis during the twisting of a Cabrol graft-right coronary anastomotic lesion 12 days after surgery. The patient was successfully treated with a primary percutaneous coronary intervention (PCI) and discharged without complications.
Case
A 52-year old woman with Marfan syndrome was admitted to the emergency department complaining of acute resting chest pain for one hour. Three years prior she had undergone a total aortic arch replacement due to aortic arch dissection with descending thoracic aortic aneurysm. The patient also had a Cabrol-type Bentall operation in another hospital using a St. Jude's mechanical aortic valve for progressive severe aortic regurgitation 12 days previously. Her electrocardiogram on arrival showed ST-elevation in the inferior leads and ST-depression in the I, aVL, V3-6. She was diagnosed with acute inferior ST-elevation myocardial infarction. Initial cardiac biomarkers showed a slightly elevated troponin T of 0.15 ng/mL but were otherwise unremarkable. Though she took warfarin, the prothrombin time expressed as a normalized international ratio was 1.6 on admission. Because her initial blood pressure was too low to measure, she was started on hydration with normal saline, inotropic support and transferred immediately to the catheter laboratory for primary PCI.
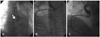
During coronary angiography, a 6 Fr EBU guiding catheter (Medtronic, Minneapolis, MN, USA) was easily inserted into the left Cabrol composite graft ostium. The left limb of the graft was found to be fully patent with normal flow {Thrombolysis in Myocardial Infarction (TIMI) grade 3} down to the left coronary artery. However, the right limb of the Cabrol composite graft ostium was not found initially. Aortic root angiography did not show the right limb of the Cabrol graft ostium. With eager, we could insert a 7 Fr multipurpose guiding catheter (Cordis, Johnson and Johnson, Cordis, Miami Lakes, FL, USA) into the right limb of the Cabrol composite graft ostium. The right limb of the graft was totally obstructed (TIMI grade 0) by heavy thrombi at the Cabrol graft to the right coronary artery (RCA) anastomosis site (Fig. 1A). Initially, we tried to aspirate with an intracoronary suction catheter using an Export aspiration catheter (Medtronic, Minneapolis, MN, USA), but it was not passed due to tortuosity. After ballooning of the anastomosis site, the whole right coronary arterial system was visible angiographically. The anastomosis site between the Cabrol graft and the RCA was significantly narrowed, angulated and twisted (Fig. 1B). An intravascular ultrasound (IVUS) study revealed a kinked and narrowed anastomotic site (Fig. 2A). Pre-dilatation was performed using a 4.0×20 mm Sprinter™ semi-compliant balloon (Medtronic, Minneapolis, MN, USA) and then a 5.0×20 mm Liberte™ (Boston Scientific, Natick, MA, USA) bare metal stent was deployed at the Cabrol graft to the RCA anastomosis site. The entire lesion including the anastomosis site was postdilated using a 5.0×8 mm Quantum™ non-compliant balloon (Boston Scientific, Natick, MA, USA). An optimal angiographic result was obtained with TIMI grade 3 flow distally (Fig. 1C). After post-dilation, the IVUS study revealed optimal stent deployment and lesion coverage (Fig. 2B). The patient was stabilized in the intensive care unit. The coronary CT angiography showed severe angulation and tortuosity between the RCA and the right limb of the Cabrol graft (Fig. 3). She was discharged five days after the primary PCI without complications.
Discussion
Although the Cabrol technique is extremely useful in cases of re-operation in which mobilization of the aortic root is made very difficult by tight adhesion,1) early 30-day mortality rates using this procedure have been reported to be as high as 20%. Recent reports showed that early 30-day mortality rates using this procedure had decreased to 4% to 11%, but overall mortality was 12% to 22%.12)13) In contrast, a button technique showed 1.9% early mortality.14) So, the Cabrol technique should be used rarely and only when a button technique is not feasible.4) Although Coronary stenosis after a Bentall procedure is uncommon, occurring in less than 2% of patients, the main concern with the Cabrol technique is maintaining the patency of the Dacron interposition grafts.7-10)13)15-18) Kim13) reported that 4 cases (44.4%) of Dacron interposition graft stenosis were observed in patients undergoing a Cabrol procedure. These lesions have usually been managed surgically15-17) although some reported cases have been managed by PCI.7-10) One of the important causes of early in-hospital mortality is acute thrombosis of the coronary grafts. This can be one of the causes of early onset sudden death.1)4) However, there have been no reported cases that have been managed by PCI in acute coronary graft thrombosis.
The pathogenic mechanism of thrombus formation in Cabrol grafts is unclear. However, our case suggests the possibility of thrombus formation. Because the right limb of the Cabrol graft was too long, it may have kinked, produced a size discrepancy and slow flow, and formed a thrombus in the anastomosis site. Another possible explanation is insufficient anticoagulation therapy after the operation. Therefore, meticulous management of a Cabrol graft anastomosis site, and sufficient early postoperative anticoagulation is warranted.
This is the first report of acute ST-elevation myocardial infarction that developed due to thrombi in a kinked Cabrol coronary graft twelve days after operation. The patient was successfully treated with primary PCI. This is just a short term result. Because the patient transferred to a surgical hospital, we only did follow up with her by telephone. She has had no major cardiac event over one year of follow up. For patients who undergo a Cabrol procedure, the main concern is maintaining the patency of the Dacron interposition grafts. Close follow-up is warranted.


 XML Download
XML Download