

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Dilated cardiomyopathy, which mostly has an idiopathic etiology, or is caused by genetic inheritance or infection, can cause irreversible congestive heart failure. Hypocalcemia is a rare etiology of reversible dilated cardiomyopathy.1-4) Here, we report a case of dilated cardiomyopathy secondary to hypocalcemia that originated from a nutritional vitamin D deficiency induced rickets in an infant who was exclusively breast-fed by a mother who had vitamin D deficiency.2-4)
Case
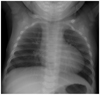
The patient was a 2 month-old girl with cyanosis, irritability, respiratory difficulty, poor oral intake and seizure-like movements, and had cardiopulmonary resuscitation on arrival. Her body weight was 5.6 kg (5 percentile). She was born at 38 weeks of gestational age with a birth-weight of 2.8 kg. She had been exclusively breast-fed. There were no medical or familial histories except an admission at an age of 10 days for hypocalcemic tetany. She was treated with calcium replacement therapy for a week. There were moist rales on both middle lung fields and chest wall retraction without cardiac murmurs or hepatomegaly. The patient had frequent episodes of muscular tetany. A chest X-ray showed an apparent cardiomegaly and pulmonary congestion (Fig. 1). An echocardiogram revealed a markedly enlarged left ventricular cavity and a hypokinetic ventricular wall motion. Left ventricular end diastolic diameter (LVDd) was 38 mm, left ventricular end systolic diameter (LVDs) was 35 mm, ejection fraction (EF) was 17%, and fractional shortening (FS) was 8%, without any structural abnormalities (Fig. 2). Electrocardiography showed sinus tachycardia (heart rate 191 beat/min), and normal QTc (0.415 seconds) (Fig. 3). Initial portable electroencephalography (EEG) showed a multiple, epileptic form discharge. Arterial blood gas analysis were pH 6.988, pO2 325.9 mmHg, pCO2 31.0 mmHg, and HCO3 7.3 mmol/L under a 40% O2 mask. Hypocalcemia as total serum calcium was 5.8 mg/dL, hyperphosphatemia as inorganic phosphorus was 10.9 mg/dL, and alkaline phosphatase was elevated (643 IU/L). Creatine kinase was 544 IU/L and creatine kinase-muscle and bone was 33.3 ug/L. Other chemistries and electrolytes studied were in the normal range. Hormone levels that were changed included elevated parathyroid hormone (155 pg/mL; normal 12-72 pg/mL), decreased 25-hydroxy vitamin D (2.6 ng/mL; normal 9.1-37.6 ng/mL) and decreased 1α,25(OH)2 vitamin D (9.2 pg/mL; normal 20.1-46.2 pg/mL). There were no metabolic disorders by amino acid and organic acid tests. Tests for viral infection were not performed. A fluorescence in situ hybridization study for chromosome 22q11 deletion was negative. A left wrist X-ray revealed mild fraying signs. After calcium and vitamin D replacement, the patient showed rapid reductions in hypocalcemic tetany, and a rapid recovery of cardiac function and cardiomegaly on chest X-ray (Figs. 4 and 5). Follow-up EEG revealed improvements as there was no evidence of epileptiform discharges. The patient was discharged on the 15th hospital day and followed up by the outpatient department with calcium gluconate and calcitriol replacement.
The mother had a vitamin D deficiency as indicated by a decreased level of 25-hydroxy vitamin D (4.3 ng/mL). Her bone densitometry study revealed osteomalacia.
Discussion
The most common cause of dilated cardiomyopathy is an idiopathic etiology (>60%), followed by familial cardiomyopathy and acute myocarditis. Other causes of dilated cardiomyopathy include viral infections, endocrine disorders and metabolic diseases.5)6) Cardiotoxic drugs and systemic diseases can also cause dilated cardiomyopathy. On arrival, our patient's serum chemistries revealed extremely low calcium and vitamin D levels. After calcium and vitamin D replacement, abnormal findings of calcium and vitamin D were corrected rapidly with the normalization of parathyroid hormone and left ventricular function recovered. In this case, electrocardiography showed normal QTc (0.415 seconds) despite severe hypocalcemia, which was due to a rapid heart rate of up to 190 beats/min (Fig. 3). Therefore, hypoparathyroidism and pseudo-hypoparathyroidsm were recorded as the cause of the hypocalcemia.7)8) The common causes of late onset hypocalcemia in the neonate are as follows; transient hypocalcemia due to maternal hypercalcemia, congenital hypoparathyroidism (ex. DiGeorge syndrome), maternal vitamin D deficiency, phosphorus overloading, renal dysfunction, hypomagnesemia, chronic diarrhea and so on.5-8) Throughout the hormonal tests, the confirmative diagnosis was congestive heart failure with dilated cardiomyopathy as a severe manifestation of hypocalcemia that resulted from vitamin D deficient rickets.




 XML Download
XML Download