

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Coronary artery aneurysm is an uncommon disease. The incidence ranges from 0.3% to 4.9% in angiographic studies.1) A coronary artery aneurysm is characterized by abnormal dilatation of a localized or diffuse segment of the coronary artery tree.2)3) The most common cause of coronary artery aneurysm is atherosclerosis. Nonatherosclerotic causes are not common. Inflammatory and connective tissue disorders account for 10-20% and include Kawasaki disease, Takayasu arteritis, polyarteritis nodosa (PAN), systemic lupus erythematosus, and Ehlers-Danlos syndrome. Other reported causes include infectious diseases such as Lyme borreliosis, septic emboli, and syphilis. The remaining causes are congenital and iatrogenic.4) The present report describes a rare case involving a young woman who presented with acute myocardial infarction (AMI) due to coronary artery occlusion related to multiple huge aneurysms and stenotic lesions in PAN.
Case
A 31-year-old female presented with acute severe chest pain lasting for more than 30 minutes at rest. The patient had experienced several recent episodes of chest pain that lasted for a few minutes and subsided spontaneously. She had no history of diabetes mellitus or smoking. However, she had been diagnosed with hypertension 3 months earlier and was being treated with medication. She had no family history of any heart disease. She denied having had any febrile disease or weight loss within the previous several months. She also denied having experienced any febrile disease accompanied by chest pain (suggestive of Kawasaki disease) in her childhood. Physical examination revealed no neuromuscular weakness, tenderness or skin abnormalities.
An electrocardiogram on admission revealed a sinus rhythm and ST-segment depressions in precordial leads V1-V6. Serum cardiac enzyme levels showed a rise in creatine kinase-MB to 121.2 ng/mL and in troponin-T to 1.73 ng/mL. Transthoracic echocardiography revealed severe hypokinesia in the inferior and posterolateral segments of the left ventricle (LV). Under the impression that the patient had had an AMI, she was initially treated with standard medical therapy, including acetylsalicylic acid 100 mg/d, clopidogrel 75 mg/d, atenolol 25 mg/d, captopril 37.5 mg/d, and intravenous heparin.
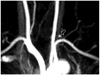
Coronary angiography revealed huge multiple aneurysmal changes involving the left main and all three major coronary arteries. The left circumflex (LCx) artery was totally occluded at its ostium and critical stenotic lesions were found at the distal left anterior descending (LAD) artery, and the posterolateral branch of the right coronary artery (RCA) (Fig. 1). There was delayed antegrade coronary filling with contrast, as well as swirling and segmental backflow of contrast in the huge aneurysms. Tc-99m myocardial single photon emission computed tomography (SPECT) revealed a small sized, severe, partially reversible defect in the apex and a moderate sized, severe, partially reversible defect in the basal lateral wall of the LV.
Laboratory test findings were as follows: white blood cell count 15.7×109/L (neutrophil 75%, eosinophil 0.3%), hemoglobin 11.6 g/dL, C-reactive protein 4 mg/dL, erythrocyte sedimentation rate 31 mm/h, rheumatoid factor 3 IU/mL, complement component 3 (C3) 93 mg/dL, and C4 16 mg/dL. Fasting plasma glucose, blood urea nitrogen (BUN), serum creatinine, albumin, liver enzymes, and lipid profile were all within normal limits. Antinuclear antibody, c-anti neutrophil cytoplasmic antibody (c-ANCA), and p-ANCA were all negative. Hepatitis B virus tests for surface antigens or antibodies all yielded negative results. Urine analysis was also normal. The serum globulin level was not measured.
Further imaging studies were performed to rule out systemic involvement of vasculitis. Brain magnetic resonance angiography showed a small aneurysm arising from the left thyrocervical trunk (Fig. 2). Computed tomographic angiography demonstrated a small aneurysm at the posterior division of the left renal artery (Fig. 3).
Although the present case did not fully meet the diagnostic criteria for PAN, the systemic involvement of medium-sized arteries with typical aneurysmal changes in a young female patient strongly suggested the presence of PAN. The patient was treated with high-dose steroids (prednisolone 60 mg/d) and an immunosuppressive agent (cyclophosphamide 100 mg/d) in addition to the aforementioned standard cardiac treatments for 2 weeks in the hospital. After discharge, the dose of cyclophosphamide was continued, but the dose of prednisolone was continued for 1 month and then progressively tapered. The patient did not develop further episodes of chest pain during hospitalization and remained asymptomatic without complications six months after discharge from the hospital.
Discussion
This case report describes a young female patient who presented with AMI and showed multiple aneurysmal deformations as well as stenotic and occlusive lesions in the coronary arteries. AMI is very rare in young Korean women. In such cases, non-atherosclerotic processes such as coronary embolism, vasospasm, dissection or vasculitis should be considered as a cause of AMI.
PAN is a systemic necrotizing vasculitis that mainly involves small- and medium-sized arteries. Secondary changes in involved arteries are common and include characteristic aneurysmal formation, intravascular thrombosis, and segmental luminal narrowing. The evolution of multiple vascular aneurysms was the most typical angiographic finding of PAN. Multiple aneurysms are identified in 60-80% of patients, but they can be encountered in other forms of vasculitis.5)
Classic PAN may involve almost any organ system. Involvement of a particular organ system includes: renal failure or hypertension in renal involvement; peripheral mono- or polyneuropathy in peripheral nervous system involvement; exercise-induced angina, AMI, or congestive heart failure in cardiac involvement; and abdominal pain, nausea, vomiting, or gastrointestinal (GI) hemorrhage in GI involvement.
The proximal and middle segments of the RCA are the most common sites for coronary artery aneurysm, followed by the proximal LAD and LCx arteries.2)6) Involvement of all three major coronary arteries or the left main stem is very rare.7) Although the evolution of multiple aneurysms is the most typical coronary angiographic finding for PAN, rare cases of coronary dissections have been reported.8)
The American College of Rheumatology (ACR) criteria for the classification of PAN include any three or more of the following ten items: weight loss greater than 4 kg, livedo reticularis, testicular pain or tenderness, myalgias, mono- or polyneuropathy, diastolic blood pressure greater that 90 mmHg, elevated BUN or serum creatinine levels, presence of hepatitis B reactants in serum, an arteriographic abnormality, and the presence of a granulocyte or mixed leukocyte infiltrate in an arterial wall biopsy.9) The initial presentation of our patient fulfilled only two items among the ACR diagnostic criteria: diastolic blood pressure greater than 90 mmHg and an arteriographic abnormality. A biopsy was not performed because of the absence of skin or neuromuscular involvement. However, some of the clinical features in our patient, including angiographically confirmed coronary artery lesions, evolution of vascular changes, young age, and being female, matched the characteristics of PAN. Other etiologies of coronary aneurysms such as Kawasaki disease, Behçet's disease, Takayasu arteritis, giant cell arteritis, or syphilitic arteritis were less likely and were not supported by the patient's medical history, physical findings and laboratory data. Atherosclerosis, the most common cause of coronary aneurysms in adults was also excluded due to the absence of risk factors.
Without treatment, the 5-year survival of patients with PAN is 13%. With optimal therapy, the 5-year survival increases to approximately 80%.10) Currently, the recommended treatment of PAN is prednisone 1 mg/kg/day for 4 weeks with subsequent tapering over 9 months and cyclophosphamide at 1.5 to 2 mg/kg/day for 1 year.11)12)
There is still no consensus on how coronary lesions related to PAN should be treated. In the present case, we did not perform a percutaneous coronary intervention because myocardial SPECT showed only minimally reversible ischemia in the LCx area and the patient did not complain of recurrent chest pain. Instead, we treated the patient medically with standard cardiac treatments. In addition, she was given aggressive antiinflammatory therapy with high-dose steroids and cyclophosphamide. The patient did not develop further chest pain and remained event-free.


 XML Download
XML Download