

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Transcatheter closure of secundum atrial septal defect (ASD) with Amplatzer Septal Occluder® (ASO, AGA medical corporation, Golden Valley, MN, USA) has become an effective and reliable alternative therapy to operation in most patients with ASD.1-6) Compared with surgical repair, transcatheter closure is safer and more physiologic, and the treatment results are similar, and as a result, transcatheter closure has surfaced to replace operation in recent years.3-5)
Owing to its design, the ASO can even be used in patients with large ASD associated with deficient rims. However, the major problem in closing a large ASD is malalignment of the device to the plane of defect. The delivery system of AGA Amplatzer has a rigid coupling between the delivery wire and the right atrial disk, which accounts for the relatively perpendicular orientation of the left atrial disk to the atrial septal plane.7)8) This character of the device results in the prolapse of the left atrium (LA) disk to right atrium (RA) during deployment (Fig. 1). There have been many efforts to overcome limitations derived from the inherent design of the ASO delivery system and many have succeeded using technical modifications.9-13) The purpose of this study is to investigate the relating factors to the need of technical modification in transcatheter closure of large ASD (≥25 mm) and to evaluate the relevant morphologic characteristics of atrial septal rim in these patients.
Subjects and Methods
Subjects
A total of 312 patients underwent transcatheter occlusion of secundum ASD with ASO at Yonsei Cardiovascular Center from July, 2003 to May, 2007. Among them, 109 (35%) patients (male 34; female 75) had more than 25 mm sized ASD and these patients were enrolled in the study. The patients were divided by the methods of deployment of ASO into two groups as group I, standard method group, and group II, modified method group. When the initial attempt of standard method failed, modified method was applied.
Echocardiographic and cardiac catheterization parameters
Assessments of the defects were measured by balloon-occlusive diameter (BOD) and its surrounding rims were based on transesophageal or intracardiac echocardiography, performed at the time of closure. The measurement of defect size based on BOD was performed according to the previous report.14) The analysis of the echocardiographic studies were performed according to the recommendations of the American Society of Echocardiogrphy.15) Echocardiographic studies were performed and images were acquired and digitally stored for offline analysis with each study by experienced physicians. Anteroinferior (AI) rim was measured as the distance to atrioventricular valve, posterosuperior (PS) rim was measured as the distance to superior vena cava, posteroinferio (PI) rim was measured as the distance to inferior vena cava, and anterosuperior (AS) rim was measured as the distance to aortic posterior wall. The two total septal lengths, anteroposterior septal length (APSL) and superoinferior septal length (SISL) was also measured and calculated. APSL was the total length between PS, ASD, and AI, and SISL was the total length between PI, ASD, and AS. AS rim was measured in the short-axis view, PS and PI rims were measured in the long-axis view or the bicaval view. AI rim was measure in 4-chamber view. In some of the cases, combinations of different views were used to determine the rim length. Any rim length was considered deficient if its length was less than 5 mm (Fig. 2).
Results
Characteristics of subjects
The profiles of the enrolled patients are summarized in Table 1. The mean age of the patients in group I was 34.7±15.5 years, 24 were male and 50 were female, the mean weight was 56±13.2 kg, the mean height was 158.8±13.1 cm, and the mean body surface area (BSA) was 1.55±0.24 kg/m2. The mean age of patients in group II was 32.9±13.6 years, 10 were male and 25 were female, the mean weight was 56.4±12.0 kg, the mean height was 159.2±12.9 cm, and the mean BSA was 1.58±0.23 kg/m2. The mean BOD size in group I and group II were 29.4±4.1 mm and 32.2±3.8 mm, respectively. The mean device size in group I was 29.4±4.0 mm and the mean device size in group II was 32.3±3.44 mm. The Qp/Qs in group I and II were 2.35±0.63 and 2.63±0.94, respectively. There were no differences between the 2 groups in age, body weight, sex ratio, and height. Group II showed a larger BOD and device size, which was statistically significant (p<0.01). Qp/Qs ratio in group II was larger than group I, but it wast statistically insignificant. In the 35 patients who underwent modified techniques, 21 patients underwent right upper pulmonary vein (RUPV) technique,9) 9 patients underwent left upper pulmonary vein (LUPV) technique,7) 3 patients underwent dilator assisted technique,16) and 2 patients underwent balloon-assisted technique.10)
Morphologic characteristics of atrial septal rims
The morphologic characteristics of the atrial septal rim in the enrolled patients are shown in Table 2. In group I, the mean PS rim length was 13.1±4.9 mm, the mean AI rim length was 15.5±5.3 mm, the mean PI rim length was 11.2±6.1 mm, and the mean AS rim length was 6.4±4.1 mm. In group II, the mean PS rim length was 12.7±4.3 mm, the mean AI rim length was 13.5±4.3 mm, the mean PI rim length was 12.7±4.2 mm, and the mean AS rim length was 2.5±2.6 mm. The mean length of AS rim in group II was significantly shorter than group I (p<0.01), but none of the other parameters showed significant difference. The mean APSL in group I and group II were 51.3±7.6 mm and 51.7±8.1 mm, respectively, and the mean SISL in group I and group II were 63.1±8.9 mm and 66.2±10.2 mm, respectively. Both APSL and SISL did not show any statistical difference between both groups.
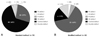
In group I with standard method, 48 patients (65%) had central defect and 20 patients (27%) had AS defect, shown in Fig. 3A. In group II with modified method, only 6 patients (17%) had central defect, whereas 22 patients (63%) had AS defect, shown in Fig. 3B. In both groups I and II, 54 patients had central defect and 42 patients had AS defect. When the patients with ASD had sufficient rims, 87% of procedure was successfully performed by standard method and 13% needed modified technique, but with AS rim deficiency, modified techniques were needed in 53% of the procedures (Fig. 4). Furthermore, as the size of the device used in the procedure increased, there was a tendency towards increase in the frequency of use of modified methods (Fig. 5).
Discussion
Many factors contribute to the difficulty involved in transcatheter closure of large secundum ASD. Over the course of time, alternative techniques of device deployment have improved, making more ASD amendable using ASO, but they still remain a challenge.
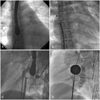
Numerous alternative techniques have been reported to facilitate transcatheter closure of large secundum ASDs,11) and our institute utilizes many of the reported modified techniques. The LUPV technique (Fig. 6A), which can be used in both children and adults, is engagement of LA disk within LUPV, followed by a rapid release of the waist and RA disk.7) The RUPV technique (Fig. 6B), recommended, but not limited, to larger patients, is partial deployment of LA disk in RUPV while maintaining contact with the posterior superior septum, followed by quick and successive deployment of the waist and RA disk.9) In the above 2 methods, it is important to place the LA disk exactly in pulmonary vein and the procedure must be performed with gentle movements until the deployment of RA disk, to avoid damage to the atrial wall. Dilator assisted technique, also known as Wahab technique (Fig. 6C), is using a long dilator, usually the delivery sheath being used, to hold the LA disk inside LA, preventing it from prolapsing across the defect.16) The balloon-assisted technique (Fig. 6D), first describe by Dalvi et al.10) in 2005, has a concept similar to the Wahab technique, but uses the balloon catheter to support the LA disk from prolapsing across the defect. These 4 techniques are the most popular modified techniques used and they were used in our patients who were enrolled in the study. In our institute, the RUPV method is the most frequently applied technique.
Our study revealed that the proportion of AS rim deficiency was higher in patients with modified methods, modified methods were needed more frequently in large-sized ASD. Therefore it demonstrated that AS rim deficiency and the size of ASD may be the core relating factors to the need of technical modification in transcatheter closure of ASD. There have been many studies describing the different modified techniques used in large ASDs,7)9)10)16) but our study is the first to analyze the factors involved in the decision of whether to employ the modified technique or not. With the prediction of a possible need of modified technique, the interventionist may be able to prepare, prior to the procedure, which may increase the success rate of the procedure. Also, by preparing, the procedure time may be reduced, which in result may moderate the complications engaged with long procedure time.
Our study was limited to patients of a single institute and only limited interventionists were involved. Further investigation with a larger pool of patients involving diverse interventionists with different techniques is pertinent in the future.
In conclusion, our study revealed that AS rim deficiency and the size of ASD may be the 2 most important relating factors to the need of technical modification in transcatheter closure of ASD. Therefore, when the initial attempt with standard method is not successful, we suggest that changing strategy of implantation may save time and efforts and possibly reduce the risk of complications associated with prolonged procedure.






 XML Download
XML Download