

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The B-type natriuretic peptide (BNP) is synthesized predominantly by cardiac ventricular myocytes, the expression of which is regulated by changes in intracardiac pressure and/or stretch. Cardiac BNP gene expression and plasma levels generally increase in patients with heart failure (HF), myocardial infarction, hypertension, left ventricular (LV) hypertrophy, pulmonary hypertension, and renal failure.1) However, we have managed some patients with elevated concentrations of the BNP and no evidence of HF, hypertension, or renal dysfunction. Thus, we report an interesting case of a young female patient with an elevated plasma level of the BNP.
Case
A 19-year-old female patient presented for evaluation on 7 April 2008 of non-specific chest pain of 1 month duration. She had no history of hypertension, diabetes, or renal dysfunction. The physical examination was unremarkable. She had worked for 6 months in a cellular phone factory. There were no abnormal findings on the electrocardiogram, echocardiogram, and treadmill test. The serum cardiac markers were within the normal range. The results of the complete blood count, blood chemistry, and urinalysis were within normal limits; however, the BNP level was 3,354.84 pg/mL. The BNP level was rechecked the next day, and was still elevated (3,079.29 pg/mL). Ten days later the BNP level was 2,982.31 pg/mL. On 30 June 2008 she was admitted to our hospital due to atypical chest pain. The physical examination was unremarkable. There were no abnormal findings on the chest X-ray, chest computed tomography, whole body scan, and coronary angiography with a spasm stress test. There were no regional wall motion abnormalities on the left ventriculogram and LV end-diastolic pressure was 10 mmHg. The laboratory findings, including a complete blood count, blood chemistries, a pregnancy test, the antinuclear antibody titer, a peripheral blood smear, and a urine test were all normal, except for a high plasma level of BNP (3,437.80 pg/mL).
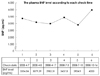
Pulmonary function testing showed that spirometry was within normal limits. She was discharged on diltiazem and a diuretic and was symptom-free. During the follow-up, the BNP level was measured twice as an outpatient and was persistently elevated (2,904.1 pg/mL and 4,000 pg/mL) (Fig. 1).
Discussion
The BNP is synthesized and secreted primarily from LV cardiomyocytes in response to increasing wall stress, particularly during diastole.2) Cleavage of the precursor peptide (proBNP) produces BNP and the corresponding amino-terminal component (NT-proBNP), which are secreted in a 1 : 1 ratio and can be detected in the peripheral circulation.3) The plasma levels of these peptides correlate strongly with each other. The BNP is bioactive and has a shorter half-life as a result of clearance by neutral endopeptidase and natriuretic peptide C-type receptors. Thus, levels are lower than for the more stable NT-proBNP.4) The levels of both peptides increase with LV pressure or volume loading, and reflect the severity of LV dysfunction. In addition, the levels of both peptides correlate inversely with LV ejection fraction and positively with increasing LV mass and indices of LV filling pressure.5) There is wide inter-individual variation in BNP and NT-proBNP levels. Up to 80% of inter-individual variation in peptide levels is explained by LV and diastolic functions, right ventricular dysfunction, renal function, age, and mitral regurgitation.6) Although Baggish et al.7) previously reported the possible causes of NT-proBNP elevation unrelated to HF, such as heart muscle disease, valvular heart disease, atrial arrhythmias, anemia, critical illnesses, ischemic stroke, and pulmonary heart disease syndromes, the patient presented herein had none of the these causes. Hereditary factors may be responsible for a significant proportion of residual variation in BNP levels.8) In this interesting case, the patient has no remarkable findings to account for the high levels of the BNP. We therefore suggest that hereditary factors may be responsible for a significant proportion of residual variation in BNP levels and further studies are required to describe the basis and need for treatment (if any) of elevated BNP levels in such patients.
 XML Download
XML Download