

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Takayasu's arteritis can affect the ostia of the left main and right coronary arteries.1-3) Involvement of a coronary artery is associated with chronic inflammation, premature atherosclerosis, and systemic vasculitis. A coronary artery bypass graft (CABG) with internal thoracic arteries is not used because the internal thoracic arteries are also involved in the inflammatory process and the subclavian arteries are occluded. Large saphenous venous grafts are usually grafted from the aorta to the affected coronary artery.4)5) Percutaneous coronary intervention (PCI) with a bare metal stent (BMS) has been performed successfully in patients with Takayasu's arteritis, but there is a high rate of restenosis due to inflammation.6)7) There is limited data available on PCI with drug-eluting stent (DES) in patients with coronary involvement secondary to Takayasu's arteritis.1)3) We describe a patient with Takayasu's arteritis involving the ostia of three large coronary arteries who was successfully treated by PCI with DES and had a good clinical outcome after 12 months.
Case
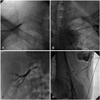
A 37-year-old male with unstable angina was admitted to our cardiovascular center. The patient had Takayasu's arteritis and an aortic valve replacement with a metallic valve due to severe aortic regurgitation 7 years previously. The patient had no risk factors for cardiovascular disease, such as diabetes mellitus, hypertension, hypercholesterolemia, alcohol abuse, or smoking. He had mild claudication in the right leg. There was no history of immunosuppressive drug use. The blood pressure was 70/40 mmHg in an arm and 120/80 mmHg in a leg. The right and left radial pulses were not palpable. An electrocardiography (ECG) revealed a left ventricle hypertrophy pattern; there were T wave inversions at V3-V6, I, and aVL, and ST segment depression in II, III, and aVF. The cardiac enzymes were normal (troponin-I, 0.01 ng/mL; and creatine kinase-MB, 3 mg/L). The 2-D echocardiography showed an ejection fraction (EF) of 44%, the left ventricle end diastolic dimension (LVEDD) was 68 mm, the left ventricle end systolic dimension (LVESD) was 56 mm, and there was a mild decrease in left ventricle systolic function and global hypokinesia. Coronary angiography (CAG) showed a 95% discrete eccentric luminal narrowing at the ostium of the large left anterior descending (LAD) and left circumflex (LCX) arteries, and 99% discrete eccentric luminal narrowing at the ostium of the large right coronary artery (RCA) (Fig. 1). The diameter of each coronary artery was >5 mm. The right and left subclavian arteries were completely occluded (Fig. 2A and B). There was no stenosis noted in the left and right carotid arteries. The ostium of the right renal artery had 80% luminal narrowing (Fig. 2C). The right superficial femoral artery was totally occluded with flow through a number of collateral vessels (Fig. 2D). The erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level were 72 mm/h and 8.2 mg/dL, respectively.
Based on the clinical and angiographic findings, the patient was diagnosed with Takayasu's arteritis. We recommended CABG, but the patient did not want to undergo surgery. We delayed PCI because the disease was in an active stage. The patient was treated with prednisolone (60 mg/day) for 14 days. The ESR and CRP decreased to 32 mm/h and 1.2 mg/dL, respectively, after 2 weeks of treatment. An intra-aortic balloon pump (IABP) was used prior to the PCI. The ostium of the RCA was predilated with an undersized balloon {4.0 mm×20 mm at 8 atmosphere (atm)}. A large 5.0×12 mm paclitaxeleluting stent (TAXUS Liberte; Boston Scientific, USA) was implanted at 16 atm (Fig. 3A). The ostia of the LAD and LCX arteries were sequentially predilated with an undersized balloon (4.0 mm×20 mm at 8 atm). Two large paclitaxel-eluting stents were implanted from the distal left main coronary artery to the LAD and LCX using the kissing stent technique (LAD, 5.0 mm×24 mm at 14 atm; and LCX, 5.0×16 mm at 14 atm) (Fig. 3B, C and D). An intravascular ultrasound (IVUS) showed good apposition of the kissing stents with minimal overlapping from the distal left main coronary artery to the LAD and LCX (Fig. 3E and F). The patient was discharged 5 days later on warfarin, aspirin, clopidogrel, a beta-blocker, a statin, nitrate, and prednisolone. There was no discomfort except for skin ecchymoses. We performed a follow-up CAG, two-dimensional (2D) echocardiography, and IVUS 6 months later. The CAG did not show restenosis or recurrence of coronary artery disease (Fig. 4A and B). The IVUS showed little neointimal proliferation and stent malapposition in the distal part of the LAD stent (Fig. 4C and D). The 2D echocardiography showed that the EF was 52%, the LVEDD was 64 mm, and the LVESD was 50 mm with global hypokinesia. We decreased the dose of prednisolone. The patient took 20 mg of prednisolone after discharge without complication. There no adverse clinical event after 12 months.
Discussion
Takayasu's arteritis is an idiophatic large vessel vasculitis that is characterized by involvement of the aorta and its major branches. Clinically, cardiac involvement is manifested as dyspnea, palpitations, angina, myocardial infarction, heart failure, and sudden death. Of patients with Takayasu's arteritis, 10-30% develop coronary artery stenosis and an even greater number of patients develop aortic valve dilatation and regurgitation due to the sustained high vascular resistance.8)9) Involvement of coronary arteries is associated with chronic inflammation, premature atherosclerosis, and systemic vasculitis. Narrowing of the coronary arteries mainly develops due to the progression of the inflammatory process of the intima and contraction of the fibrotic media and adventitia from the ascending aorta.10)
The optimal method of revasculariztion for coronary involvement of Takayasu's arteritis has not been determined. The presence of ostial coronary artery disease with concomitant inflammation of the aorta and subclavian arteries makes the decision regarding the best therapeutic approach extremely complex. The optimal method of revascularization and timing for treatment has not been established. Internal thoracic arteries are not used in CABG procedures because internal thoracic arteries are also involved in the inflammatory process and subclavian arteries are occluded. Large diameter saphenous venous grafts are usually grafted from the aorta to the coronary artery.4)5) CABG is difficult because active inflammation and severe calcifications are usually involved in the aorta of patients with Takayasu's arteritis;10) therefore, PCI could be beneficial. PCI with BMSs in patients with Takayasu's arteritis has been performed successfully, but is associated with high rates of restenosis due to inflammation.6)7) Using a DES has a potential therapeutic benefit in Takayasu's arteritis due to its local anti-inflammatory properties and resulting decrease in neointimal hyperplasia. There is limited data regarding PCI with DES in patients with Takayasu's arteritis;1)3) however, the short-term clinical results are favorable and there are no recurrences. DES has a risk of late stent malapposition, stent thrombosis, and long-term antiplatelet therapy. The long-term effects of DES in the coronary arteries of patients with Takayasu's arteritis are unknown.
In the case herein, we considered CABG using saphenous veins due to occlusion of subclavian arteries in the active inflammatory phase, but the patient did not want to undergo surgery. We therefore delayed PCI to reduce inflammation in the coronary arteries with immunosuppressive therapy. The optimal time for PCI in the active inflammatory phase of Takayasu's arteritis is unknown. It is best to defer surgery until the patient is in a non-active phase of the disease.11-14) In the case described herein, the three coronary arteries were very large in size, especially the left main coronary artery (>9 mm). We placed minimally overlapping kissing stents from the distal left main coronary artery to the LAD and LCX to reduce malapposition in the left main coronary artery. A follow-up IVUS showed stent malapposition in the distal part of the LAD stent. We suspect that the inflammatory process in the coronary arteries was involved in the ostial lesions, forming an aneurysm, and in the current case, leading to stent malapposition in the distal part of LAD stent. We do not have any data regarding the long-term prognosis of stent malapposition in patients with Takayasu's arteritis. Long-term dual antiplatelet therapy and adequate immunosuppressive therapy may be helpful for this patient.
In conclusion, PCI with DESs for patients with significant coronary involvement secondary to Takayasu's arteritis may be an effective and alternative treatment when coronary bypass grafting is not option. Long-term clinical follow up is required and the clinical outcomes of more cases managed with DES to establish the safety and efficacy of DESs in the coronary artery involvement of Takayasu's arteritis.



 XML Download
XML Download