

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Natriuretic peptides are frequently used in diagnosing and monitoring patients with congestive heart failure (CHF). B-Type natriuretic peptide (BNP) and aminoterminal pro-brain natriuretic peptide (NT-proBNP) are believed to correlate with the severity of heart failure symptoms and objective measures of heart function.1-3) The NT-proBNP levels are affected by demographic variables such as age, gender, and ethnicity, and clinical characteristics such as hypertension, atrial fibrillation, and renal function.4-6) Elevated body mass index (BMI) and obesity have been associated with hypertension, insulin resistance and dyslipidemia, and contribute to deleterious hemodynamic and morphologic cardiovascular changes.7-9) Recent studies demonstrated that obesity is associated with decreased levels of NT-proBNP and raised concerns about the diagnostic and prognostic validity of natriuretic peptides in obese patients.10)11) NT-proBNP has been shown to be increased in patients with diabetes mellitus (DM), even in the absence of structural heart disease, and obesity frequently coexists with diabetes. Hence, variety factors should be considered to be associated with the interindividual variability of plasma NT-proBNP levels in the diagnosis and management of heart failure patients. So, our study aimed to further explore the association between elevated BMI and NT-proBNP in diabetes and the relationship of echocardiographic indexes of increased left ventricular (LV) filling pressure, LV geometry and atherosclerosis as measured by common carotid intima-media thickness (CCIMT).
Subjects and Methods
Patients with chest pain and/or dyspnea who underwent cardiac catheterization from Feb. 2006 to Nov. 2007 in Maryknoll cardiac center were enrolled. Subjects with atrial fibrillation or other significant cardiac arrhythmia and acute myocardial infarction at the time of clinical assessment were excluded. Other exclusion criteria included patients who did not provide written consent and patients with regional wall motion abnormalities; symptomatic or asymptomatic LV systolic dysfunction (ejection fraction <50%); significant valvular disease (moderate or severe valvular dysfunction); and neoplastic, hepatic, and renal dysfunction. At the time of enrollment, data were collected on each subject, including demographics, physical examination, results of unblinded laboratory testing, and self-reported medical history and active symptoms. Severity of dyspnea was based on New York Heart Association criteria. Diabetes mellitus (DM) was diagnosed if fasting plasma glucose was ≥126 mg/dL or if participants were taking insulin or oral hypoglycemic medications. Patients without DM were defined as non DM. Patients were divided into body mass index (BMI) >25 g/m2 (obese), 23 to 25 (overweight), and <23 kg/m2 (non obese) according to the guideline of the Korean society for the study of obesity. Significant coronary artery disease was considered if the stenosis was above 50% from the quantitative angiography.
Echocardiographic evaluation
Measurements of left atrial (LA) dimension, left ventricular (LV) dimension, LV end diastolic and systolic volume, interventricular septal thickness (IVSd), LV posterior wall thickness (LVPWTd) and ejection fraction were performed from 2-dimensionally targeted M-mode tracings according to the recommendations of the American Society of Echocardiography (ASE). LV mass was calculated by the corrected ASE cube formula and indexed for body surface area to obtain the LV mass index. The relative posterior wall thickness (RWT) was measured at end diastole as the ratio between the double of posterior wall thickness to the LV diastolic cavity diameter. LV hypertrophy (LVH) was defined as increased LV mass index >104 g/m2 in women and >116 g/m2 in men.12) Concentric hypertrophy was defined as LVH with increased RWT (>0.43). Concentric LV remodeling was defined as increased RWT with normal LV mass index. Eccentric hypertrophy was defined as LVH without increased RWT. Transmitral peak early (E), atrial (A) diastolic velocities were measured in the apical 4-chamber view with the sampling volume positioned at the tips of the mitral valve. The isovolumic relaxation time (IRT), isovolumic contraction time (ICT) and total ejection time was measured at the apical 5-chamber view with the sampling volume positioned between the mitral valve and the LV outflow tract as the time taken from the closure of the aortic valve to the opening of the mitral valve. The index of combined LV systolic and diastolic function (the sum of ICT and IRT divided by ejection time) was calculated which described by Tei et al.13) Tissue Doppler measurements were obtained from the apical 4-chamber view, and the sampling volume was placed at the medial (septal) and lateral corners of the mitral annulus. Early (Ea) diastolic mitral annular velocities were taken as the average of 3 measurements at each side of the mitral annulus. All echocardiograms were performed and analyzed by one observer.
Measurement of common carotid IMT
Ultrasonography of the carotid arteries was performed with a 10-MHz transducer (System Five, General Electronics Corp., Horten, Norway). When an optimal longitudinal image of the common carotid artery was obtained, it was frozen on the R wave of the electrocardiogram, and 5 measurements were taken from the far wall of the distal 1 cm of the common carotid artery. This was repeated on the other side, and the average measurement from the 2 sides was taken as the CCIMT (a surrogate index for atherosclerosis). Plaques or focal protrusions were avoided. Measurements were taken at the time of examination before laboratory analysis.
Measurement of plasma NT-proBNP levels
The NT-proBNP level was analyzed at the time of clinical assessment. For each NT-proBNP measurement, 5 mL of whole blood was collected into tubes containing ethylene diamine tetraacetic acid (EDTA) and measured using the Elecycs 2010 platform (Roche Diagnostics, USA).
Statistical analysis
All data were presented as means±standard deviation and analyzed using standard statistical software {Statistical Package for Social Science (SPSS) version 13.0, Chicago, IL, USA}. Because of the large range in NT-proBNP, analysis and results using a semilogarithmic scale is also reported. Continuous variables among the DM and the non DM group were analyzed by one-way ANOVA and variables between the two groups were compared by t-test. Discontinuous variables were compared by Chi-square test. Correlations were obtained using Pearson's method. Multivariate stepwise logistic regression analysis was performed to assess the relationship between the predictor variables such as age, gender, BMI, NYHA class, hypertension, diabetes mellitus, medications, hemodynamic and echocardiographic indexes, and creatinine. A p<0.05 was considered statistically significant.
Results
The clinical characteristics of the study population
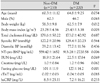
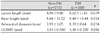
Baseline characteristics of the overall patient population are listed in Table 1. Among 933 patients, 733 were patients without DM {obese (n=287, 39.2%), overweight patients (n=216, 29.5%), and non obese (n=230, 31.4%)} and 200 were DM patients {obese (n=91, 45.5%), overweight patients (n=55, 27.5%), and non obese (n=54, 27%)}. The mean age was 60.8±10.39 years in DM patients and 64.6±8.75 years in non-DM patients. Subjects with DM tended to be older and had a higher body mass index than non-diabetes groups but had a similar distribution of gender. There was no significant difference between the DM and non-DM groups in cholesterol, systolic blood pressure, diastolic blood pressure, BUN, creatinine, and C-reactive protein. However, mean plasma NT-proBNP levels were significantly higher in DM patients than non-DM patients (913.28±2720.58 and 559.42±1652 pg/mL, p=0.006) (Table 1). Coronary artery stenosis lesion length (p=0.039), stent length (p=0.024), coronary artery adventitial diameter (p=0.034), and mean CCIMT (p=0.016) were significant higher in DM patients than non-DM patients (Table 2). In non DM patients, CCIMT was significantly higher in patients with significant coronary artery disease than patients with minimal coronary artery disease (1.23±0.568 mm vs. 1.00±0.304 mm, p=0.005). However, CCIMT showed no significant correlation with mean plasma NT-proBNP level (Table 3).
The correlation between plasma BNP level and echocardiographic findings
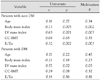
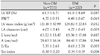
There was no significant difference between the DM and non-DM groups in LV ejection fraction, relative wall thickness, mitral E and A velocity. However, LV mass index, LA diameter, E/Ea and Tei index were significantly higher in DM patients than non-DM patients (Table 4). Plasma NT-proBNP values did not correlate with LV filling pressure represented by mitral E/Ea in obese diabetic patients (r=0.14, p=0.56). However, NT-proBNP was significantly correlated with this variable in the non obese (r=0.24, p=0.008) and non-DM patients (r=0.32, p=0.005). The significant correlation of NT-proBNP and LV mass index was observed in univariate linear regression analysis (r=0.65, p=0.001) and patients with concentric hypertrophy showed the highest NT-proBNP levels (Fig. 1). Even after adjusting for age, gender, diabetes, creatinine, ejection fraction and E/Ea in multivariate linear regression analysis, LV mass index was significantly associated with NT-proBNP (r=0.57, p=0.03) (Table 3).
The correlation between plasma BNP level and BMI
In 733 non-DM patients, plasma NT-proBNP levels were significantly lower in obese (289.62±164.9 pg/mL) and overweight patients (601.69±159.6 pg/mL) compared with non obese patients (856.39±237.3 pg/mL) (p<0001) despite similar significant coronary artery disease and severity of dyspnea (Table 5). However, in 200 DM patients, plasma NT-proBNP levels was 963.19±223.7 pg/mL, 1450.15±457.3 pg/mL, 658.05±147.1 pg/mL, respectively, which showed no significant negative correlation between BMI and NT-proBNP (r=-0.21, p=0.19) (Table 3 and 6) Drop-line charts of logtransformed mean plasma NT-proBNP levels (dependent variable) against BMI (independent) according to presence of significant coronary disease are shown in Fig. 2. Mean log NT-proBNP levels among patients with significant coronary artery disease decrease with increasing obesity, which is statistically significant in non-DM patients (5.29±1.62, 4.77±1.65, 4.53±1.43, p=0.002).
Discussion
In recent years, natriuretic peptides have been gaining widespread popularity as sensitive and specific markers for the LV failure. BNP is principally produced in the ventricles as prohormone pre-proBNP, which is then enzymatically cleaved into the biologically active BNP (32 amino acids in length) and the biologically inactive NT-proBNP (76 amino acids in length).14) It is found mainly in the cardiac ventricles, and its release appears to be directly proportional to ventricular volume expansion and pressure overload.15) BNP is an independent predictor of high LV end-diastolic pressure and the NT-proBNP levels were positively correlated with the NYHA functional class of dyspnea and the systolic dysfunction.16)17) The measurement of NT-proBNP has been reported to be a non-invasive, simple, and accurate test for older patients, obese patients, patients with chronic pulmonary diseases, and even for those patients having difficulty being tested by echocardiogram. Thus, its clinical usefulness for the differential diagnosis of heart failure is important.18)19) Elevated body mass index (BMI) and obesity have been associated with hypertension, insulin resistance and recent studies demonstrated that obesity is associated with decreased levels of NT-proBNP and raised concerns about the diagnostic and prognostic validity of natriuretic peptides in obese patients.11)20) Several potential mechanistic explanations deserve consideration. First, it is possible that the low natriuretic peptide levels in overweight and obese patients reflect less advanced stages of HF compared with lean patients.21) Cardiac cachexia, a state characterized by weight loss and neurohumoral/cytokine activation, is another potential explanation for a low BMI-high BNP association.22) Recent evidence suggests that there may be increased clearance of circulating BNP in obesity because natriuretic peptide clearance receptors are abundant on human adipocytes.23) High levels of BNP could, through their lipolytic effect, be expected to exaggerate the wasting process, which implies that a reduced BNP level in obese HF patients may be related to a decreased level of wasting. Conversely, it is also possible that overweight and obesity are associated with less robust synthesis and/or release of BNP from the myocardium.5) In the present study, NT-proBNP concentrations were lower in obese non DM patients despite higher E/Ea which has been shown to correlate with invasive measures of LV filling pressure24) and this occurs with presence of myocardial ischemia confirmed by coronary angiography. These findings have several implications. Not only do they bring into question the proper use of NT-proBNP as diagnostic tests for obese patients with volume overload, but they also raise the possibility that the decreased concentrations of natriuretic peptides may play a role in the development of heart failure in obese patients. However, the present study demonstrates that NT-proBNP is not suppressed in obese patients with DM and also shows a poor correlation with E/Ea. The mechanisms of NT-pro BNP is not suppressed in obese patients with diabetes can be explained by several possibilities. The natriuretic system and adiposity are closely linked bidirectionally.25) Lipolysis is mediated by catecholamines (stimulation of lipolysis) and insulin (inhibition of lipolysis), and natriuretic peptides have recently been shown to be important stimuli for lipolysis in humans and are similar in potency to catecholamines, and their effect is independent of both catecholamines and an insulin pathway.26) So, obese diabetic patients may have higher concentrations of natriuretic peptides compared with those without diabetes. Moreover, DM patients may be more likely to excrete NT-proBNP (and BNP) in response to a similar degree of ischemic insult,27) and then the higher NT-proBNP concentrations that we observed in patients with DM in the absence of overt HF, a finding considered to represent a "summation effect" of risk factors for structural heart disease, may still indicate an increased risk for cardiovascular morbidity and mortality.
Our present study is meaningful as we obtained the basic clinical data on the NT-proBNP test from a large study population. However, as our study was a cross-section study and the study population was not homogenous, further prospective study will be required. In addition, although the accuracy of the test was high, in some patients, their clinical results did not correlate to the NT-proBNP value. In the interpretation of the NT-proBNP test, therefore, clinical results and echocardiography must also be taken into consideration. Third, the patients with renal insufficiency were also excluded in the present study. Because, in the setting of HF, impaired renal function is common and strongly related with adverse outcomes, further study is warranted that will investigate the relationship between obesity and plasma BNP under the condition of renal insufficiency. Further studies will be required on patients showing a discrepancy between clinical features and symptoms and the NT-proBNP values.




 XML Download
XML Download