

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
With the development of anticancer drugs, radiotherapy, and the increased opportunity for bone marrow or hematopoietic stem cells transplantation, more than 2/3 of pediatric patients with leukemia or solid tumors survive long-term. The side effects following treatment, especially acute and chronic cardiac side effects after anthracycline infusion, have received considerable attention.1)2) Anthracyclines are used in more than one-half of the patients who undergo anti-cancer treatment. Recent studies have reported that the changes in cardiac function also occur in cases in which the cumulative dose of anthracycline is smaller.3)4)
The most appropriate method of assessing anti-cancer drug-induced cardiotoxicity is echocardiography, which can measure cardiotoxicity in a quantitative, non-invasive manner.5)6) Standard echocardiography assessment the global cardiac function. There are limitations with the objectivity and accuracy because a gross examination is performed in assessment of the motion and dynamics of cardiac tissue, and many environmental factors affect the measurements. The images based on Doppler are dependent on the angle of a probe, and only the velocity, the direction of which is the same as a probe, can be measured. By contrast, vector velocity imaging (VVI) is a newly-developed offline analysis. It detects changes in tissue motion at the location which was appointed by consecutive two-dimensional (2D)-image frames and thereby expresses velocity. It also includes variables in which time-dependent differential values are calculated. For this reason, in the absence of problems that several previous methods have disclosed, cardiac function can be assessed. It has been said that VVI is a superior method for analyzing tissue strain and strain rate (SR).7)8)
In the current study, we performed an analysis of cardiac function using VVI in patients who did not exhibit myocardial symptoms following anti-cancer treatment, including anthracyclines. Then, we attempted to identify the parameters showing changes in the early stage.
Subjects and Methods
Subjects
Of the patients who received anti-cancer treatment following the diagnosis of pediatric cancer at Keimyung University Dongsan Medical Center prior to 2005, 14 patients were enrolled. Their ejection fraction (EF) and fraction shortening (FS) were >56% and 29%, respectively, on echocardiography, which was performed on a yearly basis while a follow-up observation was continuously conducted until December of 2007. The patients consisted of 7 boys and 7 girls with a mean age of 9 years and 10 months (range, 6 years and 1 month-17 years and 6 months). The diagnoses included seven cases of acute lymphoblastic leukemia, three cases of acute myeloblastic leukemia, one case of neuroblastoma, two cases of non-Hodgkin lymphoma, and one case of Hodgkin lymphoma. All of the patients received anthracyclines in a protocol for anti-cancer treatment. The cumulative doses were 90-342 mg/m2. Fourteen aged-matched healthy controls were selected.
The control subjects were referred for evaluation of a heart murmur. Because of a lack of abnormal findings, the control subjects were diagnosed with innocent murmurs. The control subjects consisted of 9 boys and 5 girls, with a mean age of 9 years and 11 months (range, 7 years-15 years and 4 months). All of the subject children had a chest radiograph and an electrocardiogram.
Echocardiography
Echocardiography was performed using an Acuson Sequire 512 (Siemens Medical Solution, Mountain View, CA, USA) with a 4-MHz transducer. All of the tests that were performed were saved on the hard drive and a MO disk of the echocardiographic equipment.
On the parasternal long axis view with the use of M-mode, the FS, EF, and left ventricular (LV) mass/m2 were measured.
For diastolic functional analysis, the mitral inflow signal was acquired in the apical 4-chamber view. The pulsed Doppler sample volume was 2 mm and it was placed at the mitral valve tip. The early peak flow velocity (E) and atrial filling velocity (A) were measured three times and averaged, from which the E/A ratio was calculated. The time elapsed until the maximal E reached the baseline, the early filling deceleration time (DT), the time elapsed until the mitral valve was opened since aortic valve was closed, and isovolumetric relaxation time (IVRT), were measured.
Tissue Doppler imaging (TDI) measurements were performed on the basal septum and mitral annulus. The maximal systolic myocardial velocity (S') and early and late diastolic myocardial velocity (E', A') were measured. At this time, the sample volume was set at 3 mm. The time elapsed until the mitral valve was opened since it was closed (a') and the systolic time (b') were measured. The value of (a'-b') was divided by b', and the modified the modified (MPI) was obtained.
To analyze the VVI, the ultrasound window of the images was controlled in such a manner that the number of frames was >70 frames per single cardiac beat on the apical 4-chamber view and the 2D images were acoustically captured. The secured images were saved in a MO disk for offline analysis. With the use of an offline analysis program (Syngo US Workplace 3.0, Simence; Acuson), the contour of endocardium was manually traced on the saved images before the analysis was performed. The tracing was performed repeatedly several times for the most appropriate endocardial contour. In the septum and lateral wall of the LV, the baseline, middle part, and apex were subjected to the measurement of maximal velocity, strain, SR, and displacement. The contour of endocardium was secured in such a manner that the LV was passively drawn. This was confirmed by the visual display mode of the velocity images.
All of the echocardiographic parameters which were obtained for pulsed wave Doppler and TDI were measured by a single investigator from three cardiac cycles, and then averaged. The parameters which were obtained from the VVI were the average value from the measurement, which was performed twice.
Statistical analysis
All the results which were measured using echocardiography were expressed as the mean±standard deviation (SD). Statistical analysis was performed using Statistical Package for Social Science (SPSS) for Windows, version 14.0 (SPSS Inc., Chicago, IL, USA). A comparison of echocardiographic measurements in the septum and lateral wall of the LV between the patient and control groups was made with the use of an independent t-test. An inter-group analysis was performed using oneway analysis of variance (ANOVA), which was followed by a post-hoc analysis using Scheffe's test. A p<0.05 was considered statistically significant.
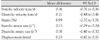
Parameters of VVI confirmed intraobserver variability. The mean difference and 95% confidence intervals between the first and second measurements were calculated.
Results
Intraobserver variability
The mean difference and 95% confidence intervals of the parameters of VVI are represented in Table 1.
An analysis of cardiac function using 2D and standard Doppler methods
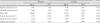
There were no significant differences in FS, EF, and LV mass/m2 measured using M-mode between the patient and control groups. DT and IVRT were longer in the patients than the controls but the differences were not statistically significant. E, which was measured using pulsed wave Doppler, was significantly lower in the patients than the controls (p=0.048); however, A and E/A did not show a significant difference (Table 2).
An analysis of cardiac function using tissue Doppler imaging
S', E', and A' in the basal septum, and S' and E' in the lateral mitral annulus, were higher in the patients than the controls but this was not statistically significant. By contrast, A' in the lateral mitral annulus was higher in the patients than the controls (p=0.027). There was no significant difference in E'/A' between the two groups. E/E' and the modified MPI were all significantly lower in the patients {in the basal septum (p=0.031 and p=0.037, respectively), and in the lateral mitral annulus (p=0.016 and p=0.041, respectively) (Table 3).
An analysis of cardiac function using the vector velocity imaging
The parameters which were obtained and then averaged from the VVI independent of location, such as cardiac velocity in the systolic and diastolic phases, strain, and SRs in the systolic and diastolic phases, were higher in the controls than the patients; however, there were no significant difference in these parameters between the two groups (Table 4).
A comparison of the regional wall functions of the ventricular septum and the lateral wall of the LV was made, and this revealed a significant difference between the patients and the controls (Table 5). In both groups, the cardiac velocity in the systolic and diastolic phases were lower in the ventricular septum than the lateral wall (p<0.001 and p=0.001, respectively). However, there were no significant differences between the two groups. The strain and SRs in the systolic and diastolic phases were not significantly different between the ventricular septum and the lateral wall in the controls. In the patients, however, the strain and SRs in the systolic and diastolic phases were lower in the ventricular septum than the lateral wall (p<0.001, p=0.011, and p<0.001, respectively). The displacement had a lower value in the ventricular septum in both groups (p=0.006 and p=0.001, respectively); however, there was no significant difference between the two groups.
In comparison to the lateral wall function of the LV between the two groups, it revealed no significant difference between the two groups. However, in comparison to the ventricular septum function between the two groups, the SRs in the systolic and diastolic phases were significantly lower in the patients (p=0.042 and p=0.010, respectively) (Fig. 1).
Discussion
Anthracyclines are effective drugs that have been frequently used to treat pediatric patients with leukemias or solid tumors, but can produce cardiotoxicity relative to the cumulative dose.1)2) Cardiotoxicity can be divided into acute (immediately after treatment), chronic (within 1 year following treatment), and late (>1 year following treatment). Higher cumulative doses and more rapid rates of drug administration have been shown to lead to an increased incidence of late cardiotoxicity.9) In cases in which the period of follow-up observation elapsed over 2 years, such echocardiographic findings as FS, the thickness of the ventricular wall, and the ventricular dimension showed abnormal findings.10) The proportion of pediatric cancer patients who develop cardiotoxicity following treatment with anthracycline is 5-10% during a mean period of 10 years (range, 2-19 years).11) Subclinical dysfunction of the LV, which was confirmed using endomyocardial biopsy, has been reported to be more common, with an incidence of 20-75%.2)9)12) According to recent studies, although the cumulative dose of anthracycline was decreased in all the protocols of anticancer treatments using anthracycline, cardiotoxicity could not be prevented.3)4) In pediatric patients, the popular methods of diagnosing cardiotoxicity due to anthracycline do not include periodic endomyocardial biopsies or stress echocardiography. For this reason, standard and Doppler echocardiography, which can be performed repeatedly, are the major diagnostic modalities in these cases.
Previous studies have reported an analysis of cardiac function following treatment with anthracycline based on echocardiography. It has been reported that a prolonged IVRT and an increased MPI following treatment with anthracyclines could be effectively used to make a diagnosis of cardiac toxicity due to anthracycline.13-15) Ganame et al.4) analyzed cardiac function 5 years following completion of treatment and classified patients in whom the cumulative dose was <300 mg/m2 into a low-dose group. Then, the authors noted that all the patients had no clinical symptoms and normal EF however, the IVRT was prolonged, abnormal pulmonary venous flow patterns developed, the end systolic wall stress was increased, the LV annular motion was reduced, and the longitudinal and radial peak systolic SR and strain were decreased on the long and short axes. Based on these findings, it was concluded that the changes in cardiac function were identified in the systolic and diastolic phases. According to another study, following anti-cancer treatment using anthracycline, myocardial velocity, which was measured using a TDI study, showed no significant changes in long-term survivors; however, the transmyocardial velocity gradient from the endocardium to the pericardium, which can be said to be an indicator of SR, showed a significant change in the ventricular septum and posterior wall of the ventricle.16) The changes in cardiac function due to the use of anthracycline were initiated from part of the myocardium, the degree of which was also very small. Therefore, an analysis of the global cardiac function did not identify these changes as promptly as possible.
In the current study, the cumulative dose of anthracycline was <300 mg/m2 in 13 patients and >300 mg/m2 in 1 patient. All of the patients were clinically asymptomatic and at least 3 years passed since the treatment was completed, corresponding to a late phase effect. The outcomes that which were observed in these patients were as follows: 1) FS and EF were normal. Systolic strain and SR were decreased, and indicating a change in cardiac function in the systolic phase. In particular, SR, which was measured in the ventricular septum, was lower in the patients. This indicated that the regional cardiac function was decreased during the systolic phase in the ventricular septum. 2) Although there was a lack of statistical significance, the IVRT was prolonged. A', which was measured on the TDI study, was significantly increased and the SR in the diastolic phase was decreased. These findings indicated that cardiac function was also changed during the diastolic phase. The characteristics of the current study, in which an analysis of cardiac function was performed using the VVI, were that cardiac function was already changed, even in patients who were treated with a smaller dose of anthracycline. These changes were detected as a change in regional cardiac function rather than global function. Strain and SR, which were measured using the VVI, were changed to a more significant extent as compared with other methods of analyzing cardiac function.
Methods of measuring regional cardiac function include TDI, as previously done, and strain and SR. Strain is the method of measuring the degree of deformity. It is expressed as either the fractional or percent change from the unloaded muscle length (the original dimension) to the loaded muscle length. SR represents the strain divided by the time, which is the deformity that occurs during a certain length of time. That is, the SR represents the rate of deformity. This is used to assess cardiac synchrony, cardiac volume, and the functions of the left atrium and ventricle.17)18) The TDI is disadvantageous in that it is affected by the traction exerted by the adjacent tissue, as well as the movement of the heart. By contrast, the measurement of strain and SR with the use of VVI is advantageous in overcoming the disadvantages of TDI and measuring the amount and velocity of regional areas on 2D images both objectively and quantitatively. In the current study, there were significant changes in E, which was measured using conventional Doppler echocardiography, and A' and E/E', which were used using the TDI and the modified MPI. However, these parameters are significantly dependent on the methods of measurement, as well as the cardiac loading conditions. The E/E' and the modified MPI were decreased, which was not in agreement with previous studies,13-15) indicating that the two parameters which were measured using TDI did not accurately reflect asymptomatic cardiac dysfunction. By contrast, strain and SR using the VVI, which are not controlled by loading as compared with other echocardiographic methods and overcame several disadvantages, were significantly changed in the systolic and diastolic phases. This can be interpreted as the usefulness in measuring the changes in cardiac function compared to other echocardiographic methods.
When the changes in regional cardiac function were observed, the current study and previous study16) showed that the function of ventricular septum was changed earlier than that of lateral wall. The causes or mechanisms for this finding are difficult to explain because the endomyocardial biopsy was not performed in all cases and there were no other testing methods which reflected regional cardiac function except echocardiography.
The greatest limitations of the current study were that the number of enrolled patients was 14, which is a relatively small number, and it was a cross-sectional study in which a comparison was made without baseline data. Therefore, it cannot be concluded that the study results originated only from the use of anthracycline. Cases in which there is a defined difference in cardiac function since the diseases were diagnosed, or those in which radiation was performed with the anti-cancer treatment, were not excluded out. Secondly, the values of strain and SR which generated the significant changes were all within the presumptive normal ranges. This also restricted the application of the results to a clinical setting. Further, the function of the right ventricle (RV) was not analyzed concurrently. Additional studies are warranted to examine whether the RV is affected by anthracycline to some extent. With the use of radionuclide angiography, however, a substantial number of studies have shown that the function of the RV were normal following the administration of anthracycline.19)
In conclusion, the changes in regional cardiac function may occur prior to the emergence of changes in global cardiac function, even in asymptomatic patients who showed normal FS and EF on echocardiography and received a low-dose of anthracyclines. The more effective methods of examining this may be an assessment of strain and SR based on 2D images with the use of the VVI study. This would be a method of analyzing changes in cardiac function as early as possible. To enable a greater degree of clinical significance and application, further studies are warranted in a larger group of patients with long-term follow-up.




 XML Download
XML Download