

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
In patients with ST elevation myocardial infarction (STEMI), revascularization therapy such as primary coronary intervention (PCI) is the cornerstone treatment that reduces hospital mortality and long term mortality.1-3) Although revascularization therapy achieves complete epicardial blood flow recovery in most STEMI patients, its beneficial effects are variable and sometimes not sufficient in patients displaying a similar amount of myocardium at ischemia. Appropriate perfusion to the tissue may be hindered by deranged blood flow in microvessels with a diameter <500 µm.6) These microcirculation disturbances result from reversible functional derangement due to vasoconstriction, plugging by platelet and tissue fragments, irreversible damage due to the swelling of necrotized tissue and direct injury of microvessels by inflammatory cells in adjacent tissue.7)8)
Several parameters can be used to assess whether appropriate perfusion is achieved in the heart tissue through microvessels. Thrombolysis In Myocardial Infarction Flow (TIMI flow grade), Thrombolysis In Myocardial Infarction Perfusion grade (TMP grade) and corrected TIMI frame count can be estimated in coronary angiography after successful PCI.9) Hemodynamic parameters such as coronary flow reserve and index of microcirculatory resistance provide more physiological information concerning microvascular blood flow.10)11) But, while these methods are acceptable for academic assessments, they are impractical for clinical use. Clinically, it is more useful and convenient to monitor ST-segment resolution (STR) on electrocardiography (ECG) after successful PCI. Because STR reflects the physiology of cardiac cells, which are the final target of coronary blood flow, it may be a theological physiologic surrogate. Incomplete STR following revascularization therapy is associated with increased mortality and recurrence rate of myocardial infarction (MI), and decreased left ventricular ejection fraction. Incomplete STR also is an independent and poor prognostic factor apart from the restoration of epicardial blood flow following PCI.12)13) In previous studies, the degrees of STR have been estimated in all elevated leads and were expressed as the sum of ST resolution in all leads. However, it is onerous to measure the sum of ST resolution in the clinical practice setting. Fortunately, rapid estimation of maximal ST resolution has no difference from that of sum of ST resolution in all leads.14) Practically, knowledge of the clinical predictors of incomplete recovery of maximal elevation of ST-segment in the early stage would be helpful for screening patients at high risk for microcirculation perfusion failure and for the planning of more aggressive treatment to recover the coronary microcirculation in such patients.
Therefore, the aim of the present study was to compare clinical parameters between complete STR and incomplete STR patients that are readily evident in the emergency setting, and to determine clinical predictors in an early clinical setting for incomplete STR.
Subjects and Methods
Patients
We recruited a consecutive series of 140 STEMI patients who had undergone primary PCI at Gyeongsang National University Hospital between October, 2005 and June, 2007. Acute MI (AMI) was defined as cases in which the typical chest pain was persistently present for more than 30 minutes, elevation of ST-segment >2 mm on the precordial leads and >1 mm on the limb lead on more than two consecutive leads, and the maximal level of the cardiac enzymes creatinin kinase (CK-MB) and troponin I were elevated three times the upper limit of normal. Patients were excluded if they had a previous AMI, >12 hours of symptoms, left bundle branch block, ventricular tachycardia, ventricular fibrillation, paced or ventricular rhythm, negative T waves in fewer than two adjacent leads with maximal ST elevation or an unsatisfactory ECG image. Based on these criteria, 39 patients were excluded from the analysis. The initial laboratory findings at admission and coronary risk factors were compared between the complete and incomplete STR groups. Systolic and diastolic blood pressure, heart rate at initial admission, pre-infarction angina, door-to-balloon time, pain-to-balloon time, left ventricular ejection fraction on echocardiography during admission, infarct site on ECG, Killip class and ischemic grade of initial ECG were acquired by protocol. Among the clinical factors, "pre-infarction angina" was defined as new onset or worsening of angina within 48 hours before admission.
Analysis of electrocardiography findings
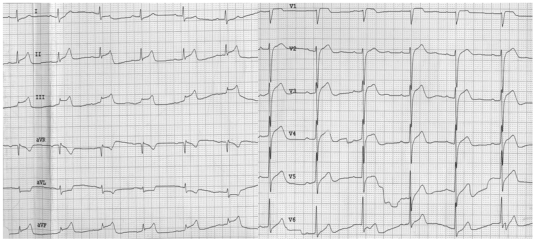
Twelve-lead ECGs at admission and 15, 30 and 60 minutes after PCI were assessed by the investigators who were blinded to the clinical characteristics and coronary angiography findings of patients. The degrees of ST-elevation were assessed by the maximal ST-segment elevation, which is similar to the sum of STR in all leads.14) Using a caliper, the degree of ST-segment elevation was assessed at the J-point of each lead from the isoelectric line (excluding aVR). STR on the 12-lead ECG at 15, 30 and 60 minutes after PCI was measured at the corresponding lead that was maximally elevated. The previous definition of complete STR as resolution >70% from maximal elevated ST segment15) was used.
The ischemia grade of each standard 12-lead ECG at admission were scored by the criteria of Sclarovsky.16) Grade 3 ischemia (G3I) was defined as the absence of a S wave below the TP-PR isoelectric line in ≥2 leads that usually have a terminal S configuration (leads V1-V3) or a ST J-point amplitude >50% of the R-wave amplitude measured from the TP-PR baseline in >2 of all other infarct-related leads (Fig. 1). Patients meeting the ST-elevation criteria but not the grade 3 ischemia criteria were classified as having grade 2 ischemia(G2I) (Fig. 2).
An assessment of coronary angiography
The location and number of lesions with significant extent of stenosis (≥50%) on coronary angiography were compared between complete and incomplete STR. After primary PCI, the blood flow recovery in the infarct-related epicardial artery was assessed by TIMI flow grade.17)
Statistical analyses
Continuous variables were expressed as mean±standard deviation (SD) and were compared using the unpaired t-test. Categorical variables were expressed as the frequency and were compared using Fisher's exact or Chi-square tests. To identify the independent factors that could predict incomplete STR, multivariate logistic regression analysis was performed for the following parameters: hypertension, duration of the chest pain, location of myocardial infarction, Killip Class, ischemia grade on ECG at the admission, initial level of troponine I and brain natriuretic peptide (BNP) and TIMI flow grade before PCI.
Statistical analysis was performed using Statistical Package for the Social Sciences (SPSS)-PC 12.0 (SPSS, Chicago, IL, USA). A value of p<0.05 was considered statistically significant.
Results
Clinical factors
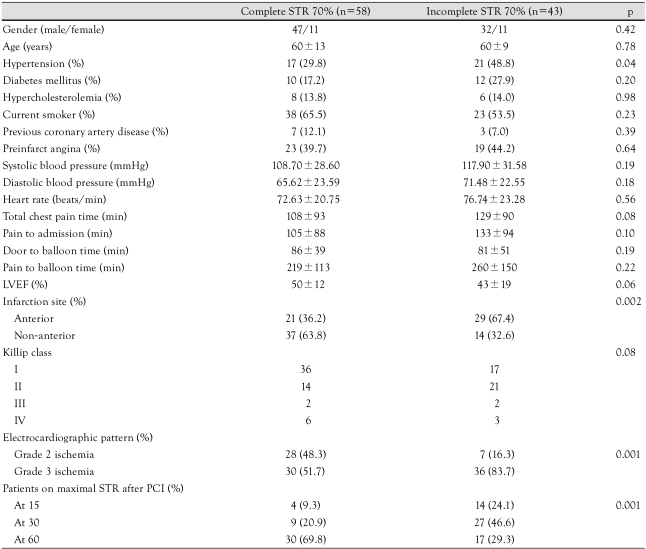
Between the two groups, there were no significant differences with respect to age and the male-to-female ratio. In regard to risk factors of developing coronary artery diseases, hypertension was significantly higher in the incomplete STR group (p<0.04). However, there were no significant differences in numbers of patients with diabetes mellitus, hyperlipidemia and tobacco smokers. No differences were apparent in the numbers of patients with preinfarction angina, mean of systolic and diastolic blood pressure and heart rate at admission. Although the incomplete STR group had a longer tendency in the total duration of chest pain (p=0.08), symptom-to-door time and door-to-balloon time were not different between the two groups. Incomplete STR group showed relatively lower tendency of the left ventricular ejection fraction (p=0.06), higher tendency of Killip class grade (p=0.08) and more frequent anterior myocardial infarction (p=0.002). The incomplete STR group also showed more frequent grade 3 ischemia (p=0.001). Resolution time of ST-segment was delayed in the incomplete STR group (p=0.001) (Table 1).
Laboratory findings at admission
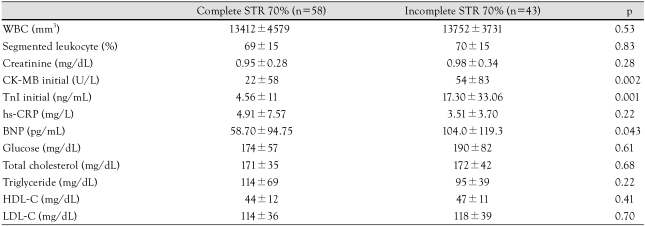
The levels of CK-MB, TnI and BNP were significantly higher in the incomplete STR group (p<0.002, p<0.001 and p<0.043, respectively). However, laboratory markers indicative of the severity of inflammations {white blood cell count (WBC), proportion of segment neutrophils, high sensitivity-C reactive protein (hs-CRP)} did not show a significant difference between the two groups (Table 2).
Angiographic findings and clinical outcome
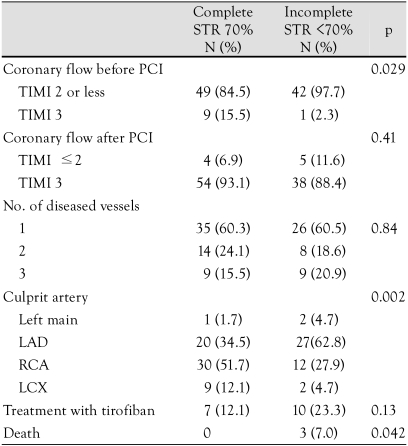
TIMI flow grade 3 before PCI was significantly evident in the complete STR group (p=0.029). Successful recovery of TIMI flow grade 3 after PCI was similar in both groups. The location of culprit lesions was more common in the left anterior descending branch in the incomplete STR group, but more common in the right coronary artery (p=0.002) in the complete STR group. The three deaths that occurred were all in the incomplete STR group (p=0.042) (Table 3).
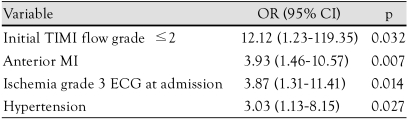
Predictors for incomplete ST-segment resolution
TIMI flow grade 2 or less before PCI was the most important independent prognostic factor for incomplete STR. Anterior wall myocardial infarction, grade 3 ischemia on ECG and hypertension were independent predictors for incomplete STR (Table 4).
Discussion
Our results indicate that TIMI flow grade 2 or less was the most crucial independent prognostic factor for an incomplete STR as a practical marker representing an incomplete recovery of microvascular flow to cardiac tissue after primary PCI. Anterior wall myocardial infarction showing elevation of ST-segment on the precordial lead, grade 3 ischemia on initial ECG and presence of hypertension were other independent prognostic factors. However, the inflammatory markers assumed to be the crucial for microvascular damages, including WBC counts and hs-CRP showed no difference in incomplete STR group compared to the complete STR group.
A previous study reported that 86% of patients showed recovery of TIMI flow grade 3 after pPCI, and old age, lower systolic blood pressure and the presence of blood clots in culprit coronary lesions were independent prognostic factors for recovery of TIMI flow grade 3.18) Our study also showed recovery of TIMI grade 3 in 91% of the patients. However, complete STR in the early stage was achieved only in 57% of total patients. These results confirmed that although PCI was successfully performed, a significant portion of patients with AMI after PCI suffer from inadequate microvascular perfusion to the cardiac tissue in the early stage in incomplete STR. STR has been reported to be a more powerful prognostic factor beyond recovery of epicardial blood flow.19) Therefore, STR in the early stage may be a convenient marker to predict the prognosis of AMI patients after PCI, and must be measured after PCI.
Microvascular damage due to the ischemia has been proposed to be classified into two types based on the pathophysiology, time and clinical significance in patients with STEMI.20) One type is the structural microvascular damage present within the necrotized cardiac muscle, which cannot be recovered due to the irreversible damage of microvascular wall. The other type is the functional microvascular damage where the anatomical microvessels are intact, but there is a vascular constriction due to endothelial dysfunction or the changes in the sympathetic nervous system, compression of microvessels due to the edema within the tissue and the microvascular obstruction due to platelets or neutrophils. In these cases, recovery of microvascular blood flow could be made by the intensive treatment. Early STR could be an important indicator discriminating between structural and functional microvascular damage. Furthermore, selection of patients judged as incomplete STR by prognostic factors will allow more aggressive treatment and an expected better clinical outcome.
TIMI flow before PCI has been significantly correlated with TIMI flow grade 3 and myocardial blush grade 3 after PCI, infarction size, left ventricular ejection fraction prior to the discharge and one-year mortality.21) The same authors reported a significant correlation (p=0.009) between TIMI flow grade before PCI and recovery of ST-segment.22) Consistent with these studies, we presently confirmed that the maintenance of blood flow prior to the procedure or a spontaneous recovery of ST-segment as powerful independent factors for a recovery of ST-segment.
Previous studies have demonstrated that the proportion of cases in which there was a TIMI flow grade 3 prior to PCI was approximately 20%.23)24) Early restoration of coronary blood flow is achieved by the spontaneous dissolution of clots, which can be promoted by drugs as aspirin, other ADP blockers and heparin. Our result also emphasizes that the development of drugs and treatment regimens capable of improving blood flow prior to PCI is most important for reducing microvascular damage in the patients with STEMI.
As compared with non-anterior wall MI, the degree of STR was lower in anterior wall MI with precordial ST elevation. Other studies have reported similar results.25)26) To date, little is known about the exact mechanisms. In one study, the degree of correlation between the mortality and incomplete STR in anterior wall MI was found to be lower than that seen in non-anterior wall MI.27) It has been hypothesized that the degree of STR at a precordial lead is, to a lesser extent, due to previous early repolarization or left ventricular hypertrophy. Because patients with anterior wall MI commonly have a greater infarction size than at other sites, it can be inferred that the resulting severe inflammatory responses may contribute to incomplete STR.
Presently, the patients with grade 3 ischemia showed agreater size of infarction, higher mortality and higher recurrence rate than those with grade 2 ischemia. "No reflow" phenomenon after PCI is also more frequent in patients with grade 3 ischemia.27)28) This grade of ischemia could be a prognostic factor that predicts incomplete STR and inappropriate reperfusion after PCI.29) Our study confirmed that grade 3 ischemia is also an important prognostic factor for an incomplete STR. Interestingly, hypertension was also an independent prognostic factor for an incomplete STR. These results support the possibility that microvascular dysfunction is prevalent in patients with hypertension, and that a recovery of ST-segment is measured to a lesser extent in patients with hypertension who had a left ventricular hypertrophy. Left ventricular hypertrophy itself may cause ST elevation.
Based on our results, the recovery of epicardial coronary blood flow before PCI is implicated as the most important factor to prevent incomplete STR. Earlier use of anti-platelet agents such as aspirin and platelet IIb/IIIa receptor antagonist must be considered in STEMI patients, especially those at high risk with all predictors for incomplete STR. Adenosine triphosphate (ATP)-sensitive potassium channel openers that act to prevent microvascular constriction can also be useful in this setting. The use of instruments associated with thrombectomy or distal protection during PCI have displayed the more beneficial effect on coronary microvasculature.30) Therefore, these predictors for incomplete STR can be helpful in selecting high risk patients, although PCI itself can produce microvascular damage due to the migration of thrombus or plaque debris.
Our study has several limitations. First, because the study was conducted in a single-institution setting, selection bias may influence the results. Secondly, although STR is useful and easy to measure, it can not be a standard and accurate indicator for the microvascular damage unlike invasive hemodynamic parameters. Further studies utilizing hemodynamic factors such as coronary flow reserve and index of microcirculatory resistance or recovery of corresponding wall motion abnormalities as an indicator for microvascular damage are warranted. Studies using these parameters will further our understanding of STR as a indicator of microvascular damage, which has advantage and limitation.

 XML Download
XML Download