

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia and a major cause of substantial mortality and morbidity from stroke, thromboembolism, and heart failure, leading to an impaired quality of life.1-5) With the increase of elderly population in the developed world, the prevalence of AF is increasing, resulting in a major public health problem.6) Maintenance of sinus rhythm is the main therapeutic goal in patients with AF.
Radiofrequency catheter ablation (RFCA) for AF has been proposed as an effective therapeutic option for AF that is resistant to pharmacologic rhythm or rate control, with successful long-term maintenance of sinus rhythm in the absence of treatment with anti-arrhythmic drugs reported in the majority of patients.7) However, the recurrence of AF after RFCA is not uncommon. The recurrence rate of AF after RFCA has been reported to be between 30 and 40%, depending on the ablation strategy and the type of AF.7-10) Some investigators have reported that the left atrial diameter/volume and hypertension are predictors of AF recurrence after RFCA.11)12)
Recent research has focused increasingly on atrial structural remodeling and electrical dysfunction, which underlie the development of AF in different pathologic conditions.13-17) A particular interest has been generated in the role of renin-angiotensin system (RAS) blockade in reversing the electrical and structural remodeling of diseased atria.
Angiotensin-converting enzyme inhibitors (ACEIs) are known to suppress structural and functional remodeling and prevent the induction and promotion of AF in chronic rapid atrial pacing dogs.18) In several animal models, it has been suggested that angiotension II type 1 receptor blockers (ARBs) might be useful for preventing AF recurrence after the termination of sustained AF by decreasing interstitial fibrosis.19)20) However, there is still uncertainty about the role of ACEIs and ARBs for the reduction of AF recurrence after RFCA in clinical practice.
This study was aimed to evaluate the effect of ACEIs and ARBs on the recurrence of AF after RFCA.
Subjects and Methods
We retrospectively evaluated 152 patients (mean age, 57±10 years; M : F=94 : 58) who underwent AF ablation due to drug-refractory paroxysmal (mean age, 57±10 years; M : F=58 : 43) or persistent AF (mean age, 56±10 years; M : F=36 : 15).
Among the 152 patients, 101 had paroxysmal AF (PAF) and 51 had persistent AF (PeAF). PAF was defined as the occurrence of two or more episodes of AF during the previous 12 months, typically lasting <7 days and terminating spontaneously. PeAF was defined as the occurrence of AF episodes lasting <7 days, and typically requiring cardioversion for restoration of normal sinus rhythm. The AF ablation strategy was 3D mapping (CARTO)-guided circumferential ablation, pulmonary vein ostial ablation, and roof line, mitral valve isthmus, and right cavotricuspid isthmus block. AF ablation techniques were identical for all patients.
After discharge, the patients were followed 1-2 weeks later, and then visited our hospital every 1-3 months during the first year after RFCA. Whenever the patients visited our clinic, a history was taken and a physical examination was performed. Additionally, a 12-lead electrocardiography (ECG) and 24-hour ambulatory Holter ECG monitoring (24 hours Holter monitoring) were obtained. Thereafter, we immediately checked a 12-lead ECG and 24 hours Holter monitoring if the patients complained of symptoms, such as palpitations that suggest AF. Twenty-four hours Holter monitoring was also performed on asymptomatic patients every 6 months.
Recurrence was defined if the patients showed AF on a 12-lead ECG and/or on 24 hours Holter monitoring, or complained of typical episodes of palpitation sat the 3-month follow-up visit after RFCA.
We compared the recurrence rates between the PAF and PeAF groups that received ACEIs or ARBs. ACEIs or ARBs were prescribed at least 1 month prior to ablation and for the duration of the follow-up. We used the standard doses that are generally recommended for ACEIs or ARBs. The mean follow-up duration was 18±14 months.
Statistical analysis
The Statistical Package for Social Sciences (SPSS) for Windows, version 15.0 (Chicago, IL, USA) was used for all analyses. The continuous variables are presented as the mean values±standard deviations (SDs) and were compared using paired or unpaired Student's t-tests. A p<0.05 was considered statistically significant.
Results
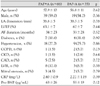
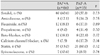
The PAF and PeAF groups, with or without ACEIs or ARBs, were similar with respect to important baseline clinical characteristics (Table 1 and 2). Furthermore, there was no difference in medications, including anti-arrhythmic drugs other than ACEIs/ARBs for the PAF and PeAFFgroups (Table 3 and 4).
The overall recurrence rate after ablation therapy was 26% (n=39). In PAF patients, no significant differences existed in the recurrence rates between the group with ACEIs or ARBs and the group without ACEIs or ARBs (24.2% vs. 22.9%, p=0.87) (Fig. 1). However, in PeAF patients, compared with the group not using ACEIs or ARBs, the recurrence rate was significantly decreased in the group using ACEIs or ARBs (12.1% vs. 61.1%, p<0.01) (Fig. 1).
In PeAF patients with and without recurrence, the left atrium dimension (44.2±8.4 mm vs. 44.3±5.8 mm, respectively, p=0.45) and the left ventricle ejection fraction (62±6.5% vs. 61.5±6.2%, respectively, p=0.28) were not significantly different.
In multivariate analysis, the use of ACEIs or ARBs was independently associated with recurrence after adjusting for the left atrium dimension and the left ventricle ejection fraction (OR=0.078, 95% CI=0.02-0.35, p<0.01).
Discussion
AF is a complex, multifactorial disease. The underlying etiology is probably different in different patient subpopulations. The paroxysms of AF are consistently initiated by a spontaneous firing focus arising from several sites, including the pulmonary veins,21-24) the vein of Marshall,25) the coronary sinus,23)26) the crista terminalis,23)26) the superior vena cava, and the inferior vena cava. The role of substrate is not as important as in PAF.
However, electrophysiologic remodeling is commonly observed and is probably an important factor contributing to the persistence of AF. In addition to eletrophysiologic remodeling, structural remodeling, such as fibrosis (at both the subcellular and tissue levels) is also often present and contributes to the altered tissue substrate that promotes AF maintenance.27)
Although there are many anti-arrhythmic drugs available to maintain sinus rhythm and reduce the ventricular rate, there is no drug which can control AF effectively.
Because RFCA can effectively treat patients with drug-refractory AF, RFCA has emerged as a major treatment option for AF. However, this procedure is limited by a significant rate of AF recurrence and the effect of RFCA on patients with PeAF is not as effective as on PAF. This phenomenon may be caused by structural and electrical remodeling of the atrium during the long period of AF.
Several experimental studies have demonstrated that atrial cells express all components of RAS in a pig model of AF,28) remodeling of the atrium correlated with a high level of angiotensin in atrial tissue, and blockade of RAS through ACEIs or ARBs can reverse atrial remodeling.13)18)29) Nakashima et al.30) first demonstrated the role of ACEIs and ARBs in preventing atrial electrical remodeling. They found that in dogs in which the atria were paced at 800 beats/min, candesartan and captopril prevented the atrial effective refractory period from shortening.
In the current study, the overall recurrence rate after ablation therapy was 26% (n=39). The recurrence rate was significantly decreased in the PeAF group that used ACEIs or ARBs (12.1% vs. 61.1%, p<0.01). This result might be caused by the effect of ACEIs or ARBs on alteration of left atrial remodeling and reduction of interstitial fibrosis through RAS blockade. However, this difference in the recurrence rate was not observed in PAF patients (24.2% vs. 22.9%, p=0.87).
We presume that the reason for this outcome might be caused by difference of pathophysiologic mechanisms between PAF and PeAF. That is to say, PAF is mainly triggered by electric foci, but electrophysiologic or structural remodeling underlie PeAF. Therefore, ACEIs or ARBs which can alter remodeling, played an important role in reducing the recurrence rate of PeAF, but not PAF.



 XML Download
XML Download