

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The incidence of coronary artery anomalies is approximately 1% among patients undergoing cardiac catheterization,1-4) 0.29% among autopsy specimens,5) and less than 0.1% among prospective echocardiographic screenings.6) Most anomalies are incidentally detected and do not create clinical problems.1-4) However, 19-33% of sudden cardiac deaths in the young population are attributable to coronary artery anomalies.7-9) An anomalous origin of the right coronary artery (RCA) from the left sinus is a very rare anomaly, and its incidence is 0.019% to 0.49% on coronary angiography.1-4) However, recent angiographic studies have reported a relatively high incidence (5.6%) of coronary artery anomalies and anomalous RCA origins from the left sinus (0.92%).10) Anomalous origin of the RCA (0.17%) is more common than anomalous origin of left coronary artery (LCA, 0.047%).1) Coronary artery anomalies are classified as benign (80.6%) but potentially serious anomalies (19.4%). Potentially serious anomalies include ectopic origin from the pulmonary artery, ectopic origin from the opposite aortic sinus, single coronary artery, and large coronary fistulae.1) These anomalies may be associated with sudden death.
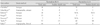
Anomalous origin of either the right or left main coronary artery from the contralateral sinus with an interarterial course between the aorta and the pulmonary trunk may also be associated with sudden death and may cause myocardial ischemia, arrhythmia, and syncope.11-19) There have been several reports concerning these anomalies and their attendant clinical problems in Korea.20-25) The incidence of anomalous RCA is higher in angiographic studies and lower in autopsy studies compared to that of anomalous LCA, which is also a more common cause of sudden death (Table 1).11-17) Anomalous LCA is more common in young male subjects,11-17) possibly because of the longer intramural course and larger area of dependent myocardium in the left ventricle.26)27) The incidence of anomalous RCA from the left coronary sinus differs among the races: the incidence in Western countries is 27%, and the incidence in Japan is 79% (44 of 56 patients). Death has not been reported in relation to this anomaly in any of the 44 Japanese patients. An interarterial course existed in 12 anomalous LCA cases.17) Study of the proximal structures, including the takeoff portion, is important in formulating a treatment plan,3)10-19)26)28-30) and many imaging tools are now available to evaluate this anomaly. Multi-detector CT (MDCT) is the favored imaging method. This review describes the pathophysiology, imaging methods, surgical methods, and treatment of anomalous RCA from the left coronary sinus with interarterial course.
Pathophysiology
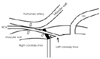
The pathophysiology of the restricted coronary blood flow seen in this anomaly is suggested to be as follows. The acute takeoff angle, slit-like orifice, and compression of the intramural segment by the aortic valve commissure are all thought to narrow the orifice. Lateral luminal compression of the intramural portion of the coronary artery and compression of the coronary artery between the aorta and the pulmonary artery are also possible mechanisms (Fig. 1).11-19)28)31)32) Some autopsy-based studies have shown that slit-like orifice structure and acute angle takeoff are more common in sudden cardiac death patients.14-16) In a MDCT-based study, acute angle takeoff was correlated with luminal stenosis of the orifice.25) However, there is still controversy concerning the mechanism by which the interarterial course is compressed between the aorta and the pulmonary artery. An intravascular ultrasound (IVUS) study26) found that luminal compression of the coronary artery was totally attributable to the aorta because the pressure of the pulmonary artery was much lower than that of the aorta. Another MDCT study showed that the narrowing of the orifice was more severe than that of the interarterial course was.25) However, the sudden cardiac death associated with this anomaly is related to severe exercise, and our study was conducted at rest, so further mechanistic evaluation is necessary.
Coronary Artery Disease and Congenital Anomalies
The correlation between coronary artery obstructive disease and coronary anomalies is uncertain. Some authors insist that anomalous coronary arteries increase the risk of coronary artery obstructive disease,33)34) but the prevailing opinion is that the anomalous portion of the coronary artery is not vulnerable to obstructive disease,4)29)35)36) The incidence of concomitant congenital anomalies is 4.2-24%; common anomalies include bicuspid aortic valve and mitral valve prolapse.3)25)
How to Evaluate
The methods used to evaluate anomalous RCAs include echocardiography, angiography, MDCT, and MRI. Noninvasive tools such as MDCT19)37-41) and MRI42-45) can provide precise information about the complex anatomy of coronary artery anomalies, though MDCT is favored due to its higher spatial resolution and rapid exam time. Additionally, MDCT can provide numerous multiplanar image reconstructions to permit precise evaluation of the takeoff portion and course of the anomalous coronary artery (Fig. 2). Transthoracic echocardiography provides limited information in this regard, and transesophageal echocardiography provides more information,22) but both of these methods are invasive. Evaluation is difficult in angiography because the complex three-dimensional structure of the anomalous coronary artery is displayed in a two-dimensional plane, and selective cannulation of the anomalous coronary artery is made difficult by the small, slit-like orifice. The success rate of selective cannulation is 55-61%.25)39)40)41) This success rate is not correlated with the takeoff angle or the orifice size or shape, so the relatively low Figure has been attributed to limited experience on the part of physicians, who rarely see this anomaly.25) MDCT-guided cannulation may be useful in increasing the success rate of cannulation. IVUS is also a useful method for obtaining cross-sectional luminal images,21) but cannulation is difficult, and this method is also invasive. MDCT provides excellent information concerning orifice location and the course of the anomalous coronary artery, so MDCT should be performed prior to angiography or IVUS. The size and shape of the slit-like orifice differ according to image projection, so multiplanar image reconstruction is necessary in precise evaluation. Angiography and echocardiography are invasive, have a relatively low cannulation success rate, and are limited with respect to multiplanar image reconstruction. Therefore, MDCT is the best method for imaging coronary artery anomalies despite its radiation. Further developments in MRI may lead to displacement of MDCT in the future.
Surgical Methods
Surgical treatment methods are variable. The unroofing procedure31)32) manipulates the orifice, enlarges the orifice, and makes an acute angulation, which decreases the lateral compression of the intramural segment. Possible serious complications of this procedure include aortic valve incompetence due to injury of the intercoronary commissure. This method does not manipulate the interarterial course and has good results. Associated findings support the suggestion that the pulmonary artery has little or no effect on the constriction of coronary blood flow. Percutaneous coronary intervention (PCI)20)46)47) relieves systolic compression, but selective cannulation and stent insertion in the anomalous RCA are difficult to perform due to the small, ectopic orifice and the long, curved intramural portion of the anomalous RCA. Prior to PCI, the anomalous RCA must be evaluated by MDCT; MDCT-guided cannulation is helpful in selective cannulation and intervention.20)21) Coronary artery bypass grafting (CABG)32)48) is technically easy because it does not entail opening of the aorta or manipulation of the intercoronary commissure. However, the native anomalous RCA is patent at rest, so obstruction of the CABG by competition flow is possible.32) Ligation of the native anomalous RCA proximal to the anastomosis is a feasible method for preventing competition flow.48) Coronary reimplantation32) of the anomalous RCA in the right coronary sinus is also useful, but the disadvantage of this method is that it carries the risk of neoostial stenosis.
Debate on Treatment Policy
Sudden death without symptoms occurs frequently in patients with anomalous LCAs, so surgical repair is recommended.16)49) However, sudden death is extremely rare in asymptomatic patient with anomalous RCAs, and there is no sudden death in children under 10 years of age or adults over 30 years of age.49) Eckart et al.9) reported 21 coronary artery anomalies related to sudden death among 6,300,000 military recruits, and all cases were anomalous LCAs from the right coronary sinus. According to the MDCT-based study of Lee et al.,25) significant stenosis (>50%) of an anomalous RCA occurred in only 1 of 24 patients, and this patient, whose symptoms disappeared after an unroofing procedure (Fig. 3), now has an outstanding acute takeoff angle and a small orifice. Other patients with more obtuse angles and mild or absent narrowing of the orifice and artery exhibit no anomaly-related problems in the absence of treatment (Fig. 2). One report has suggested that subclinical ischemic changes in the myocardium are relatively frequent (8 of 16 patients) in anomalous RCA patients in the postoperative period.50) Treatment of anomalous RCA with an interarterial course from the left coronary sinus is still debated because most anomalous RCAs are benign, with a small risk of sudden death and late myocardial ischemia after surgery is undertaken. Pelliccia7) insists on treatment as follows. Young patients (<35 years) with symptoms or ischemia should undergo surgery. In young patients (<35 years) without symptoms or ischemia, the best therapy is uncertain. Older patients without symptoms or ischemia do not need surgical therapy. Strenuous exercise should be limited. Gersony49) suggests that anomalous RCAs should be followed without intervention and believes that the benefit of excessive exercise limitation is doubtful. I agree with this suggestion and believe most patients should be followed without aggressive treatment. If a young, symptomatic patient has significant luminal narrowing on imaging studies, surgical intervention should be considered.
Conclusion
Multiplanar MDCT image reconstruction at the takeoff portion of the anomalous RCA permits precise evaluation of the takeoff angle, size of the slit-like orifice, and course of the anomalous RCA. Most anomalous RCAs with interarterial courses from the left coronary sinus are benign. Precise and thorough imaging evaluation of anomalous RCAs is necessary prior to selection of treatment method.


 XML Download
XML Download