

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Approximately 50 years ago, Dr. John H. Gibbon, Jr., performed the first successful clinical surgical procedure using the heart-lung machine, which he had developed in his research laboratory over a period of more than two decades. This accomplishment had a profound impact on the medical community, particularly on researchers in the cardiovascular field.1) In 1966, DeBakey2) reported the first successful use of a ventricular assist device (VAD) for postcardiotomy support; the patient was supported by the device for ten days. In 1969, Cooley et al.3) became the first surgeon to implant an artificial heart (designed by Liotta) in a human being.
Since the 1960s, many research groups have been involved in the development of other mechanical circulatory support (MCS) devices, including univentricular and biventricular devices, aortic counterpulsation pumps, and total artificial hearts (TAHs). Historically, these devices have been used to provide short-term support for patients in cardiogenic or postcardiotomy shock, or to bridge patients to transplantation. More recently, they have been used to provide support during high-risk interventional procedures, as a bridge to recovery, or as destination therapy.
When medical therapy fails to provide sufficient support for patients with refractory heart failure or cardiogenic shock, mechanical means of supporting the circulation are necessary. The number of patients with heart failure is steadily increasing, with an estimated 500,000 new cases recorded annually in the United States.4) The most common cause of acute refractory heart failure or cardiogenic shock is extensive acute myocardial infarction.5) Cardiogenic shock may also occur as a result of acute myocarditis, myocardial contusion, or progressive end-stage heart failure.
Mechanical Circulatory Support Devices
Device type
There are a number of ways in which MCS devices can be classified.
Class I devices are intended for very short-term use (hours to days) and are used when early functional recovery is expected and minimal intervention is desirable.
Class II devices are used when an intermediate support time is expected (days to weeks), but functional recovery is expected to take longer.
Class III devices are intended for extended use (months to years). There are three main subcategories of extended use. First, the device may be used as a therapeutic bridge to recovery (BTR) or as a means to provide a chronic boost to native function and, therefore, to provide a better exercise response and improved quality of life (QOL). Second, the device may be used as a bridge to transplant (BTT), as most of the current first generation devices have.
The third category has been variously described as destination, long-term alternative to transplantation, permanent, or definitive (DT) MCS therapy. This application is aimed at patients who are thought to have no prospect of either transplantation or of native ventricular recovery and who will be reliant on a device for the rest of their lives.
Class IIIb includes all devices that do not have direct blood contact and is further subdivided into active and passive devices.6)
Device selection
The type of VAD support depends on patient status and the length of device support anticipated.
Patients who require mechanical circulatory support can be divided into the three main categories listed below:
Profound shock: patients in acute, profound shock; for instance, those with post-cardiotomy cardiac arrest, potentially with end-organ failure and right heart failure.
Decompensating congestive heart failure (CHF): more chronically ill patients who are transplant candidates.
Non-transplant candidates: patients not at a transplant center who have potentially recoverable myocardium.7)
Catheter-Based Mechanical Circulatory Support Devices (Class I Devices)
TandemHeart
The TandemHeart left ventricular assist device (LVAD) is a left atrial-to-femoral artery bypass system that can be implanted percutaneously within 30 minutes and that provides active hemodynamic support. A 21-French venous polyurethane inflow cannula is inserted transseptally into the left atrium to aspirate oxygenated blood, and an arterial perfusion catheter returns the blood from the external pump to one or both femoral arteries. The device can remain in place for up to three weeks. Chandra et al.9) reported the initial experience with this device as a successful bridge to cardiac recovery in three patients with acute myocarditis (Fig. 2).
Impella Recover left ventricular assist devices
The Impella Recover device is a microaxial LVAD with a diameter of 6.4 mm at the body of the pump and a diameter of 7.3 mm at the level of the outflow opening.
A small electric motor is built into the device, and a thin (2.8 mm) cable leading to the device contains the electrical power supply. The power supply is connected to an external control unit, as well as a purge line connected to a purge perfusor, through which heparin is flushed continuously with a pressure of 300 to 700 mmHg.
Twenty-four Impella devices were inserted between September 2001 and March 2003. Most patients were unable to be separated from cardiopulmonary bypass. Mean pump flow was 3.3±0.7 L/min, and mean support time was 61±56 hours. Overall mortality was 54%, similar to that seen in high-risk intra-aortic balloon pump patients (Fig. 2).10)
Medos DeltaStream DP1®
The Medos DeltaStream DP1® blood pump system (Medos AG, Stolberg, Germany) is used for pumping human blood in extracorporeal circuits. This device features a diagonal-flow impeller and can be used for both continuous and pulsatile output. The DP1®, an extracorporeal rotary blood pump, is used as an extracorporeal membrane oxygenator (ECMO) and an LVAD device.
Between January 2002 and April 2006, 11 patients required ECMO support for acute postcardiotomy heart failure. Five patients were supported using a LVAD. In the ECMO group, one patient died of peritonitis, and two patients died of persistent pulmonary hypertension and major neurologic complications. In the LVAD group, one patient died of low cardiac output syndrome 9 days after weaning. All other patients were discharged. The major advantages of this device include easy implantation and straightforward management (Fig. 2).11)
Class II Devices
Abiomed BVS 5000®
BVS 5000® is a dual chamber, temporary, external pulsatile VAD powered by a pneumatic console that can operate one or both pumps simultaneously and that can be used for isolated univentricular or biventricular support.
Between April 1993 and January 2003, 71 patients underwent implantation with this device. Nineteen patients were supported with LVADs, 30 patients were supported with right ventricular assist devices (RVADs), and 22 patients were supported with biventricular assist devices (BIVADs). Overall, 29 (40.8%) patients were successfully weaned from support after myocardial recovery, including 7 (36.8%) LVAD, 13 (43.3%) RVAD, and 9 (40.9%) BIVAD patients (Fig. 3).12)
Thoratec PVAD®
The Thoratec VAD is a pneumatically driven device, which has an effective stroke volume of 65 mL and can deliver pulsatile flows of 1.3 to 7.1 liters/min. It consists of three components: (1) a blood pump, which acts as a prosthetic ventricle; (2) cannulae, which connect the blood pump to the heart; and (3) a drive console that powers the blood pump pneumatically. The pump is paracorporeal and, as such, is positioned on the anterior abdominal wall with percutaneous cannulae exit sites 2 to 4 cm below the costal margin. As of July 2006, the Thoratec MCSD system had been used in more than 2,800 patients worldwide, ranging in age from 6 to 77 years and ranging in weight from 17 to 144 kg.
Between July 1999 and January 2002, 19 patients underwent placement of a Thoratec BIVAD. Duration of BIVAD support averaged 22 days, with a range of 0 to 91 days. Fifty-nine percent of patients were successfully bridged to transplantation. Seven patients died while on VAD support, with all but one death occurring within 30 days of implantation. Four patients died from multisystem organ failure. Two patients died from sepsis. One patient died from hemorrhagic stroke. No mechanical pump failures were encountered with this device (Fig. 4).13)
As of September 2003, a total of 30 patients with advanced heart failure had been supported with the Thoratec implantable ventricular assist device (IVAD) for bridge-to-transplantation or post-cardiotomy ventricular failure in Europe and the United States.
Berlin heart (ExCor)®
This blood pump consists of a transparent polyurethane housing that is divided into one air chamber and one blood chamber by a three-layer membrane. ExCor® was first used in June 1988. As of January 2007, it had been used 1600 patients in 26 countries, of which 237 were pediatric patients. In North America, it has been used in 74 patients in 26 clinics since 2000 (Fig. 5).14)
MEDOS MCSD®
This pump is known for excellent flow features and biocompatibility. It was developed in line with the latest know-how in construction techniques and hemodynamics. MEDOS ventricles are available in different sizes, in the interest of providing optimal support for patients ranging from infants to large adults: adult HiFlux (80/72 mL), adults (80/72 and 60/54 mL), children (25/22.4 mL), and infants (10/9 mL). As of July 2006, the MEDOS system had been applied 350 times in 84 hospitals worldwide as a bridge to recovery, as well as a bridge to transplant. Patients ranged in age from 4 days to 76 years and in weight from 3 kg to 135 kg; applications were left ventricular, right ventricular, and biventricular (Fig. 5).8)
Clinical Trials for Destination Therapy (Electrical Sac Pump)
The Randomized Evaluation of Mechanical Assistance for the Treatment of Congestive Heart Failure (REMATCH) trial
The landmark Randomized Evaluation of Mechanical Assistance for the Treatment of Congestive Heart Failure (REMATCH) trial is considered one of the most remarkable endeavors in the history of clinical trials for heart failure. Between May 1998 and July 2001, 129 patients (68 HeartMate XVE and 61 maximal medical therapy) from 20 transplantation centers in the United States were enrolled in this trial. Enrolled patients were not eligible for transplantation, had received optimal medical therapy for at least 60-90 days under the care of a heart failure cardiologist, and had been declared to have a projected life expectancy of less than two years (Fig. 6).14)
The one- and two-year survival rates of 52% and 23% in LVAD recipients were significantly better than the 25% and 8% survival rates observed in control subjects treated with maximum medical therapy (p=0.001) (Fig. 6). The survival rates of LVAD recipients were better in the cohort enrolled during the second half of the REMATCH trial when compared with the early enrollment (37% versus 21% two-year survival), but there was no difference in the outcome with medical therapy throughout the trial.
The success of the REMATCH trial with HeartMate VE was followed by US Food and Drug Administration (FDA) approval of the refined model, HeartMate XVE, to be used as the first and only device for Destination Therapy in the United States.
As of July 2006, over 4,100 patients worldwide have been supported with the HeartMate MCSD.15)
The Clinical Utility Baseline Study trial
The Clinical Utility Baseline Study (CUBS) trial was the first European nonrandomized, single-arm observation study that evaluated the safety and performance of the LionHeart-2000 (LionHeart Ventricular Assist System; Arrow International, Reading, PA). The fully implantable LionHeart is powered by transcutaneous energy transfer, thereby obviating the need for external lines, which are a common source of infection in LVAD recipients (Fig. 7). The 23 patients were enrolled in the CUBS trial at seven European centers and one US transplant center between October 1999 and December 2003. CUBS patients were supported for a total of 7,980 combined implant days, with a mean implantation time of 347 days. At one year, the overall survival rate was 39%. This was lower than the survival rate in the REMATCH LVAD group (51%). However, at two years, the survival rates were roughly equivalent for both groups (22% CUBS, 26% REMATCH).
This trial demonstrated that implantable technology holds promise for use in permanently supported patients. Although there was a 68% increase in the incidence of local infections, the CUBS trial showed a 37% decrease in the incidence of sepsis and a 26% decrease in septic death. There was also a 9% decrease in device-site infections and a 100% decrease in pump-housing and pump inflow- and outflow-tract infections.16)
As of July 2006, a total of 26 patients had been implanted with the Arrow LionHeart MCSD.8)
The Investigation of Non-Transplant Eligible Patients Who are Inotrope-Dependent trial
The Investigation of Non-Transplant Eligible Patients Who are Inotrope-Dependent (INTrEPID) trial was a nonrandomized, two-arm clinical trial conducted at 13 centers in the United States and Canada with experience implanting the Novacor LVAD as a BTT. The trial was initiated in early 2001 and concluded in June 2003 with a total of 51 patients enrolled at 20 study sites in the United States. Patients treated with LVADs had superior survival rates at 6 months (46% vs. 22%) and at 12 months (27% vs. 11%) compared with patients treated with optimal medical therapy (OMT) (Fig. 8).17)
As of July 2006, more than 1,700 implantations had been done at over 90 centers worldwide. The 95 patients were supported for over one year, and 2 patients were supported for over four years.
Next Generation Devices (Axial Flow Pumps)8)
Axial pump
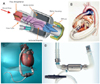
MicroMed DeBakey VAD®
The MicroMed DeBakey MCSD was projected to be 1/3 less expensive than currently marketed pulsatile MCSDs, making it more affordable to a wider group of patients.
European clinical trials began in November 1998, and the US clinical trial began in June 2000. In April 2001, the FDA expanded the clinical trial parameters to 20 clinical sites and 178 patients. As of July 2006, over 380 patients at 14 heart centers in 7 countries had been implanted with the device (Fig. 9A).
Jarvik 2000®
The Jarvik 2000 continuous flow pump is a non-pulsatile device that is much simpler and more compact than pulsatile devices, operating at 25,000 rpm. As of July 2006, over 100 patients had received this device (Fig. 9B).
HeartMate II®
The HeartMate II is a second-generation MCSD that features a miniature rotary blood pump with axial bearings. Because of its small size, the rotary blood pump may potentially be used to provide cardiac support in small adults and in children. The clinical trial was initiated in 2000 (Fig. 9C).
InCor®
InCor is the only axial system worldwide to be equipped with an active magnetic bearing that allows for a freely floating impeller; it is axially active and radially passive without producing any actual physical contact. Because of its smaller size, this pump is easily implantable. InCor was first used in clinical studies in June 2002, and it received CE mark approval in March 2003. As of January 2007, the InCor LVAD had been used in 313 patients in 15 countries (Fig. 9D).
Centrifugal pump
EvaHeart®
This pump is a third generation centrifugal pump that has a unique thromboresistant coating over its blood contacting surface. A pilot BTT clinical trial was initiated in Japan in 2005. Three patients received the device, and all survived the 98- to 164-day support period (Fig. 10A).
DuraHeart®
The DuraHeart is a centrifugal pump with a magnetically levitated impeller. As of January 2007, 29 devices had been implanted, with a mean support duration of 165 days. Eleven patients were supported for more than 6 months and four for more than 1 year (Fig. 10B).
HeartMate III®
HeartMate III is a third-generation heart assist system featuring a miniature centrifugal pump and state-of-the-art magnetic technology. This system is currently being evaluated in an ongoing animal trial (Fig. 10C).
CorAide LVAS®
The Arrow CorAide is a third-generation centrifugal titanium pump. As of July 2006, 21 implantations had been performed, with support periods of 23-400 days (Fig. 10D).
VentrAssist®
The VentrAssist has only one moving part: a hydrodynamically suspended impeller with a fully redundant back-up motor drive, controller, and processors. It weighs 298 g and measures 60 mm in diameter, making it suitable for both children and adults. The VentrAssist is currently being studied in a five-center, ten-patient US feasibility trial (Fig. 10E).
HeartWare®
This device has a diameter of 4 cm and a height of less than 2 cm, with an integrated inflow conduit. The small size of the device allows for intrapericardial placement, which reduces surgical trauma and facilitates the implant procedure. As of January 2007, seven patients had undergone implantation with HeartWare pumps and were awaiting transplantation (Fig. 10F).
Total Artificial Hearts
CardioWest®
The CardioWest has prosthetic ventricles made of polyurethane and four Medtronic-Hall mechanical valves. By the end of 2006, the CardioWest TAH had been implanted in 635 patients for a total duration of over 100 patient-years. In 2004, the CardioWest TAH received FDA approval as a BTT device (Fig. 11).
AbioCor®
The AbioCor consists of two blood-pumping chambers. The right pump supplies blood to the lungs, while the left pump provides blood to other vital organs. After implantation, the device does not require any tubes or wires to pass through the skin. The replacement heart is about the size of a grapefruit and is quiet. As of mid-November 2001, a total of 273 patient-days were accumulated with the AbioCor, with no significant problems noted. As of July 2006, fourteen patients had received AbioCor implants, and the first patient had the device in place for over 130 days (Fig. 11).
Pediatric circulatory support devices
ECMO and centrifugal pump-based VADs have been the most commonly used circulatory support modalities for pediatric patients in the United States. During the last few years, substantial advances have been made in the field of pediatric circulatory support. A number of devices suitable for pediatric patients are now available.
Survival after VAD implantation
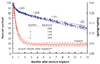
Survival after VAD implantation continues to be inferior to that achieved after transplantation, but it must be realized that many patients receive BTT device therapy because they are too ill for transplantation at the time of device implantation. Hence, this represents a considerably higher risk patient subset (Fig. 12).18)
The upper curve and the 70% confidence limits (dashed lines) represent the parametric survival curve. The individual survival points and accompanying error bars represent the actuarial depiction. The lower curve and its confidence limits represent the hazard function. Percent survival is indicated on the left vertical axis, and hazard function units are displayed on the right vertical axis. The numbers in parentheses indicate the number of patients available for follow-up at the designated time point.
The high-risk nature of this patient population is supported by the fact that multi-organ system failure remains the major cause of death (Table 2).
On multivariate analysis, the two strongest predictors of death after LVAD placement were severe RVAD and older age. The interaction between these risk factors demonstrates the dramatic increase in mortality when biventricular support is required in patients over 60 years of age.18)
The impact of age on the success of BTT therapy is shown in Fig. 13. For patients less than 30 years age, nearly 75% have undergone successful transplantation by approximately 1 year, whereas only 50% of those age 50 years or older survive to transplantation within 1 year.
Conclusions
Heart failure is now acknowledged as the most common fatal disease in industrialized countries, with advanced heart failure having a worse prognosis than most forms of cancer.19)
The International Society of Heart and Lung Transplantion (ISHLT) Registry reports that the one-year post-transplant survival rate has remained below 80% over the past 5 years, with a 5-year survival rate of about 60% and a steady attrition rate of 4% per year thereafter.20)
Over the last two decades, MCSDs have undergone rapid development, with the goal of supporting patients with advanced heart failure as a bridge to cardiac transplantation, a bridge to recovery, or an alternative to transplantation. The major current limitations to this therapy are infection, coagulopathies, and device dysfunction. Major morbidity has been declining as centers have gained wider experience in recipient management, despite the enrollment of sicker patients.
We believe that the use of LVADs in patients with advanced heart failure results in a clinically meaningful survival benefit and an improved quality of life and that LVADs are an acceptable alternative therapy for selected patients who are not candidates for cardiac transplantation.14)













 XML Download
XML Download