

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Percutaneous transluminal angioplasty (PTA) with stent implantation tends to be utilized more commonly, compared with vascular surgery, in patients with chronic symptomatic peripheral artery occlusion have not responded to conservative management. PTA has been attempted using a transfemoral approach in cases with in-stent reocclusion, which has been proposed as a considerable issue.1) However, cases undergoing PTA with a transradial approach have rarely been reported. Furthermore, there are no cases involving PTA using devices designed for percutaneous coronary intervention (PCI). We present a case herein of in-stent reocclusion of the common iliac artery using devices designed for PCI with a transradial approach.
Case
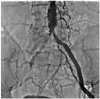
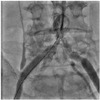
A 68-year-old man sought evaluation at our hospital for intermittent, effort-related chest pain, claudication, and discoloration of the right lower extremity. He was a 35-pack year current smoker and had diabetes mellitus for 4 years. We decided to perform a coronary angiogram for evaluation of the coronary artery disease. We failed in the right femoral artery approach due to occlusion of the right common iliac artery. Although the left common iliac artery was also narrowed, we inevitably performed a coronary angiogram with the left femoral artery approach. Therefore, we PCI was performed of the coronary artery stenotic lesions, including the proximal left circumflex artery and the proximal left anterior descending artery. We also performed PTA with a 7 mm × 6 cm self-expandable Corinthian IQ™ stent (Cordis, Miami, FL, USA) at the right common iliac artery. After the procedure, he was discharged feeling more comfortable with medications, including aspirin, clopidogrel, cilostazol, a beta-blocker, an angiotensin converting enzyme inhibitor, and a statin. Unfortunately, he refused to stop smoking. Three months later, he returned to our hospital due to the insidious recurrence of claudication, with an onset about two months earlier. The right femoral artery pulse was absent and the angiogram revealed in-stent restenosis of the right common iliac artery, in which the thombolysis in myocardial infarction (TIMI) flow was 0 (Fig. 1). In addition, contralateral access was impossible because an approach requiring an acute angle of entry with advancement of the guiding catheter through the stent struts due to the upward extension of the stent to the abdominal aorta. Thus, we adopted a right transradial approach to the lesion. Initially, we used a 100 cm, Judkin's Right™ catheter, which was too short to reach the lesion. Then, we advanced a 120 cm, 5 Fr Heartrail™ straight tip catheter (Terumo, Tokyo, Japan) to the ostium of the occluded right common iliac artery. Although we tried to advance a 0.035" guidewire (Terumo) via the right radial artery, it could not advance through the hard lesion. Therefore, we decided to use the guidewire which had been developed for PCI. Thereafter, a Conquest 9 gram guidewire (Asahi Intecc, Seto, Aichi, Japan) penetrated the occluded lesion with support of 1.5 mm over-the-wire (OTW) PCI balloon (Fig. 2). The occluded lesion was dilated with the OTW balloon and a 3.5 × 20 mm PCI balloon several times. However, we could not get an optimal luminal diameter (Fig. 3) due to the hardness and elastic recoiling of the lesion in spite of several attempts. Two days later, complete resolution of the in-stent reocclusion was accomplished by an 8 × 10 mm peripheral cutting balloon (Boston Scientific, Boston, MA, USA) via the ipsilateral femoral artery (Fig. 4), which was not available 2 days previously. He was discharged without complication with the medications mentioned above.
Discussion
Peripheral arterial occlusive disease (PAOD) of the lower extremities is an important cause of morbidity that affects up to 10 million people in the United States.2) Intermittent claudication is the most common symptom.
Greater than 70 percent of patients diagnosed with PAOD remain stable or improve with conservative management. Those who do not improve with conservative management may undergo surgery or PTA. Surgical bypass has been the gold standard for extensive PAOD. However, rapid advances in percutaneous revascularization techniques and equipments have significantly changed the patterns of vascular reconstruction. In one study, comparing PTA with bypass surgery in patients with disabling claudication and femoropopliteal stenosis, PTA increased the quality-adjusted life expectancy by 2-13 months, and resulted in decreased lifetime expenditures. Therefore, angioplasty is the preferred initial treatment in patients with disabling claudication and a femoropopliteal stenosis or occlusion.3)
Restenosis is a well-known problem after PTA. Although vascular graft surgery has been recommended in almost cases of restenosis, PTA has been attempted to reopen the reoccluded lesion recently.4)
The use of the radial artery, which was first reported by Campeau in 1989,5) has become more popular in PCI. However, cases undergoing PTA with a transradial approach have been rarely reported. The limitations of the transradial approach include difficulties in advancing the catheter due to vasospasm, anatomic variations, and a longer distance to the target lesion.6)7) Nevertheless, this approach should be particularly beneficial for patients undergoing PTA for several reasons. First, these patients frequently present with bilateral disease. Second, this approach eliminates compressing the common femoral artery after the procedure. Third, this approach facilitates same-day discharge, even in the presence of aggressive antithrombotic treatment. Although there are current limitations to the radial artery technique, the potential benefits should justify the development of specific devices designed for this purpose.8)
Conquest family wires with an OTW balloon (Asahi Intecc), which are stiff and hard, have yielded higher successful results in patients with chronic total occlusions (CTO).9) Although no case has been reported involving PTA using devices designed for PCI, we suggest that Conquest family wires can be useful in patients undergoing PTA in hard peripheral arterial occlusions.
In conclusion, a transradial approach with a long guiding catheter designed for PCI may be an alternative if the transfemoral approach is unattainable. In addition, Conquest family wires and a balloon designed for CTO in PCI may be possible solution in hard peripheral arterial occlusion.


 XML Download
XML Download