

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background and Objectives
The overall prognosis of patients with vasospastic angina (VA) is relatively good. However, the long-term prognosis and its influencing factors are not well understood in Korean patients.
Subjects and Methods
Between August 1996 and January 2007, 256 consecutive patients with VA were reviewed (215 men, 53±9 years). Coronary spasm was confirmed via intravenous ergonovine provocation in all study patients during coronary angiography. Major adverse cardiac events (MACEs) were defined as myocardial infarction (MI), resuscitation from cardiac arrest, or repeat hospitalization due to recurrent angina.
Results
The 256 patients were followed for an average of 59 months (range, 5 months to 11 years). Thirty-one patients (12.1%) were lost to follow-up. Cardiac deaths occurred in 6 patients (2.3%), non-fatal MIs occurred in 3 patients (1.2%), and MACEs occurred in 52 patients (20.3%). The rates of survival at 1, 3, and 5 years were 99%, 97%, and 97%, respectively, and the rates of MI-free survival at 1, 3, and 5 years were 99%, 96%, and 95%, respectively. Rates of MACE-free survival at 1, 3, and 5 years were 91%, 81%, and 62%, respectively. MI at initial presentation and current smoking were factors significantly associated with MACEs; these factors were also independent predictors of MACE-free survival.
Conclusion
Despite treatment with calcium channel blockers, recurrent episodes of angina were frequently observed, whereas sudden cardiac death and non-fatal MI were rare. Smoking and myocardial infarction at admission were independent risk factors for cardiac death, non-fatal MI, and repeat hospitalization due to recurrent angina in patients with variant angina.
Figures and Tables
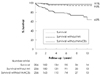
Fig. 1
Survival (top), MI-free survival (middle), and MACE-free survival (bottom) for the entire patient population (256 patients). Each point represents a cardiac death, a non-fatal MI, or recurrent angina requiring repeat admission. MACE: major adverse cardiac event, MI: myocardial infarction.






References
1. Park SJ, Park SW, Kim JJ, et al. Increased basal coronary artery tone and hyperresponsiveness to acetylcholine and ergonovine in spasm related coronary artery in patients with variant angina. Korean Circ J. 1994. 24:928–936.
2. Prinzmetal M, Kennamer R, Merliss R, Wada T, Bor N. Angina pectoris: I. a variant form of angina pectoris. Am J Med. 1959. 27:375–388.
3. Oliva PB, Potts DE, Pluss RG. Coronary arterial spasm in Prinzmetal angina: documentation by coronary angiography. N Engl J Med. 1973. 288:745–751.
4. Hills LD, Braunwald E. Coronary artery spasm. N Engl J Med. 1978. 299:695–702.
5. Sun H, Mohri M, Shimokawa H, Usui M, Urakami L, Takeshita A. Coronary microvascular spasm causes myocardial ischemia in patients with vasospastic angina. J Am Coll Cardiol. 2002. 39:847–851.
6. Ajani AE, Yan BP. The mystery of coronary artery spasm. Heart Lung Circ. 2007. 16:10–15.
7. Adlam D, Azeem T, Ali T, Gershlick A. Is there a role for provocation testing to diagnose coronary artery spasm? Int J Cardiol. 2005. 102:1–7.
8. Lanza GA, Sestito A, Sgueglia GA, et al. Current clinical features, diagnostic assessment and prognostic determinants of patients with variant angina. Int J Cardiol. 2007. 118:41–47.
9. Harding MB, Leithe ME, Mark DB, et al. Ergonovine maleate testing during cardiac catheterization: a 10-year perspective in 3,447 patients without significant coronary artery disease or Prinzmetal's variant angina. J Am Coll Caridiol. 1992. 20:107–111.
10. Bertrand ME, Lablanche JM, Tilmant PY, et al. Frequency of provoked coronary arterial spasm in 1089 consecutive patients undergoing coronary arteriography. Circulation. 1982. 65:1299–1306.
11. Sueda S, Ochi N, Kawada H, et al. Frequency of provoked coronary vasospasm in patients undergoing coronary arteriography with spasm provocation test of acetylcholine. Am J Cardiol. 1999. 83:1186–1190.
12. Sueda S, Kohno H, Fukuda H, et al. Frequency of provoked coronary spasms in patients undergoing coronary arteriography using a spasm provocation test via intracoronary administration if ergonovine. Angiology. 2004. 55:403–411.
13. Kang JA, Lee YS, Jeong SH, et al. Clinical characteristics of patients with variant angina. Korean J Med. 2002. 63:195–202.
14. Lee HC, Hong SR, Kim HS, et al. The risk factors of vasospastic angina. Korean Circ J. 2002. 32:224–232.
15. Sugiishi M, Takatsu F. Cigarette smoking is a major risk factor for coronary spasm. Circulation. 1993. 87:76–79.
16. Cheon BW, Rha SW, Wani SP, et al. Impact of smoking and smoking-related parameters on acetylcholine-induced coronary artery spasm. Korean Circ J. 2006. 36:661–665.
17. Jeong JY, Lim DS, Kang JA, et al. The study of coronary spasm by follow-up coronary angiography in variant angina. Korean Circ J. 2002. 32:791–797.
18. Ogawa H, Yasue H, Oshima S, Okumura K, Matsuyama K, Obata K. Circadian variation of plasma fibrinopeptide A level in patients with variant angina. Circulation. 1989. 80:1617–1626.
19. Takizawa A, Yasue H, Omote S, et al. Variant angina induced by alcohol ingestion. Am Heart J. 1984. 107:25–27.
20. Sueda S, Mineoi K, Kondo T, et al. Characteristics of spasm-induced vessels in patients with vasospastic angina and a history of syncope. J Cardiol. 1998. 31:331–335.
21. Takizawa A, Yasue H, Omote S, et al. Variant angina induced by alcohol ingestion. Am Heart J. 1984. 107:25–27.
22. Yasue H, Kugiyama K. Coronary spasm: clinical features and pathogenesis. Intern Med. 1997. 36:760–765.
23. Silverman ME, Flamm MD Jr. Variant angina pectoris: anatomic findings and prognostic implications. Ann Intern Med. 1971. 75:339–343.
24. Severi S, Davis G, Maseri A, Marzullo P, L'Abbate A. Long-term prognosis of "variant" angina with medical treatment. Am J Cardiol. 1980. 46:226–232.
25. Water DD, Miller DD, Szlachcic J, et al. Factors influencing the long-term prognosis of treated patients with variant angina. Circulation. 1983. 68:258–265.
26. Mark DB, Califf RM, Morris KG, et al. Clinical characteristics and long-term survival of patients with variant angina. Circulation. 1984. 69:880–888.
27. Walling A, Waters DD, Miller DD, Roy D, Pelletier GB, Theroux P. Long-term prognosis of patients with variant angina. Circulation. 1987. 76:990–997.
28. Nakamura M, Takeshita A, Nose Y. Clinical characteristics associated with myocardial infarction, arrhythmia, and sudden death in patients with vasospastic angina. Circulation. 1987. 75:1110–1116.
29. Waters DD, Bouchard A, Theroux P. Spontaneous remission is a frequent outcome of variant angina. J Am Coll Cardiol. 1983. 2:195–199.
 XML Download
XML Download