

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The maze procedure has been shown to be effective in restoring sinus rhythm (SR) in patients with atrial fibrillation (AF), both with and without identifiable underlying organic heart disease.1-9) Restoration of SR has been reported to be successful in 75% to 95% of patients who have undergone the maze procedure.1-9) Restoration of SR using the maze procedure permits the electrical activation of the atrium and the reestablishment of its mechanical function, with the possibility of reducing thromboembolic complications and improving hemodynamics.10)11) However, the rates of restoration for SR and atrial mechanical function are apparently different; the rates of restoration and maintenance of atrial mechanical function vary in the literature.6)8)9)12)13)
The aim of this study was to determine whether the restoration of SR using the maze procedure was associated with the restoration of atrial function, and to evaluate whether the preoperative left atrial volume index (LAVI) and the immediate postoperative atrial mechanical function could predict the conversion of AF to SR
Subjects and Methods
Study subjects
This study was prospectively conducted in 80 patients who underwent the maze procedure with cryoablation and concomitant valvular operation at Samsung Medical Center, Seoul, Korea, between March 2005 and February 2007. All patients had chronic AF. The term chronic AF denotes the presence of uninterrupted AF for at least 6 months, with no evidence of spontaneous reversibility to SR. Patients with sick sinus syndrome, uncontrolled hyperthyroidism, permanent pacemakers, or previous cardiac surgery were excluded from the study. The protocol was approved by the Institutional Research Ethics Committee. Written informed consent was obtained from all participants, and the recommendations of the revised version of the Declaration of Helsinki were met.
All patients had mitral valve disease: 40 patients had mitral stenosis, 34 patients had mitral regurgitation, and 6 patients had combined mitral stenosis and mitral regurgitation. No patients were being treated with antiarrhythmic agents (class I, II, III, or IV) or digoxin at the time of the study. The maze procedure was performed simultaneously in conjunction with the following procedures: mitral valve replacement (mechanical valve, n=57; tissue valve, n=4) and mitral valve repair (n=19) (Table 1).
Hypertension was defined as repeated SBP measurements of ≥140 mmHg or DBP measurements of ≥90 mmHg, or previous antihypertensive drug treatment. Diabetes mellitus was defined as a serum glucose level of 125 mg/dL or higher, a history of diabetes mellitus, or current anti-diabetic therapy. Thyroid dysfunction was defined as a diagnosis of hyperthyroidism or hypothyroidism. Current smoking was defined as cigarette-smoking within one year prior to the maze procedure.
Maze procedure
The operative procedure used for all patients in our study was fundamentally the same as that initially described by Cox and associates. The exception was we used cryoablation to create the linear lesion pattern and the lesions in specific areas guided by direct visualization.6)9) All procedures were performed through median sternotomy, using cardiopulmonary bypass with bicaval venous drainage under moderate hypothermia and cardiac arrest. Concerning the valve operation, the valve was excised first, and then the maze procedure was performed, followed by valve replacement or reconstruction. Neither atrial appendage was excised. Cryoablation lesions were created endocardially with a custom-made 4 mm-long handled T shape and a 6 mm-long straight Cryoprobe (EP Technologies, Boston Scientific Corp, San Jose, CA). Cryo-generators were set at -60℃. Each cryoablation was delivered for 160 seconds to achieve a transmural lesion. Lesions were made to isolate the pulmonary veins with the posterior left atrial wall in conjunction with the left atriotomy incision by encircling them all in one and connecting the isolated area by creating lines to the mitral annulus. Right-sided cryoablation lesions were applied inferior to the coronary sinus, from the tricuspid annulus to the left atriotomy site. If the right atrium was large, or if tricuspid valve incompetence was significant, another right-sided lesion was made from the right atrial appendage to the tricuspid annulus. Thereafter, the left atrial appendage was oversewn within the left atrium.
Echocardiography
Transthoracic echocardiographic examinations were performed in all patients with a 2.5 MHz transducer attached to a commercially available Doppler echocardiography machine, before and immediately after the maze procedure (<2 weeks), then 6 months after the procedure. M-mode measurements were performed in accordance with the recommendations of the American Society of Echocardiography. In addition to routine M-mode measurements of left ventricular function, the mitral inflow velocity was recorded with pulsed Doppler. The Doppler sample volume was placed at the tip of the mitral valve leaflets as they opened, or at the center of the mitral prosthesis. The tissue Doppler of the mitral annulus was obtained from the 4-chamber apical view in the septal position. Left atrial volume was determined using the prolate ellipse method averaged over five beats: diameter 1 was the anteroposterior dimension measured from the parasternal long axis view; diameter 2 and diameter 3 were the width (or minor axis) and the perpendicular length (or major axis) of the 4-chamber view, respectively. Left atrial volume was calculated using the following formula: 0.523×diameter 1×diameter 2×diameter 3. Left atrial volumes were determined at end-systole (just before opening of the mitral valve) and end-diastole (just before mitral valve closure). The volumes were indexed by body surface area. Atrial mechanical function was assessed by means of left atrial ejection volume (LAEV) and left atrial ejection fraction (LAEF). LAEV was calculated as follows: indexed LA end-systole volume-indexed LA end-diastole volume. LAEF was calculated as follows: (indexed LA end-systole volume-indexed LA end-diastole volume) / indexed LA end-systole volume×100.14)15)
Postoperative management and follow-up
Cardiac rhythm was monitored continuously for 48 hours. Thereafter, daily 12-lead electrocardiograms (ECGs) were performed during hospitalization. Per protocol, all patients stopped their anti-arrhythmic medications after undergoing the maze operation. Amiodarone was started in patients who developed persistent AF during the hospital stay. Electrical cardioversion was attempted in patients who remained in AF. Warfarin was administered to all patients for the duration of the study, and all patients underwent transthoracic echocardiography before hospital discharge. Patients were seen at 1, 3, and 6 months postoperatively in the outpatient clinics, where they underwent clinical examination and 12-lead ECG. Transthoracic echocardiography was also performed at 6 months. If a patient reported symptoms suggestive of arrhythmia either at a specified follow-up visit or between visits, a 24-hour Holter tape (and an ECG if appropriate) was obtained. Likewise, findings on any sporadic ECGs obtained by the patients' primary physicians were taken into account. At 6-month follow-up, 71 patients remained in SR, and 9 patients had persistent AF, despite medical and electrical cardioversion.
Statistical analysis
Statistical analysis was performed using SPSS Pc+12.0 software. The student's t-test was used to compare the mean subgroup values, and the Chi-square test was used to compare the categorical variables. Pearson's correlation was used to estimate the correlation between two variables. For the receiver operating characteristic (ROC) curve, we used MedCalc version 4.20 (Frank Schoonjans, Belgium). Differences were considered statistically significant when p were less than 0.05.
Results
The clinical characteristics of the study population are shown in Table 2. The mean patient age was 54.4±11.6 years. Of 80 enrolled patients, 44 patients (54%) were women. At 6-month follow-up after the maze procedure, 71 patients remained in sinus rhythm (SR group). However, AF did not convert to SR after the maze procedure in 9 patients (AF group). There were no significant differences in age, sex, hypertension, diabetes mellitus, renal failure, stroke, hyperthyroidism, hypothyroidism, or smoking history between the groups.
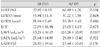
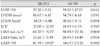
Table 3 shows the echocardiographic findings before the maze procedure. There were no significant differences in left ventricular ejection fraction (LVEF), left ventricular internal diameter in diastole (LVIDD), left ventricular internal diameter in systole (LVIDS), E/E', LAEV, or LAEF between the groups, but the AF group exhibited significantly higher LAVI than did the SR group (p=0.010). Table 4 shows the echocardiographic findings immediately (<2 weeks) after the maze procedure. There were no significant differences in LVEF, LVIDD, LVIDS, E/E', LAVI, LAEV, or LAEF between the groups. Table 5 shows the echocardiographic findings 6 months after the maze procedure. There were no significant differences in LVEF, LVIDD, LVIDS, E/E', LAEV, or LAEF between the groups, but the AF group had significantly higher LAVI than did the SR group (p=0.008).
Fig. 1 shows the changes in LAVI, LAEV, and LAEF before and after the maze procedure in the SR group and the AF group. The changes in LAVI, LAEV, and LAEF were significantly different between the both groups. LAVI decreased gradually during the follow-up period in the SR group. In the AF group, LAVI decreased in the immediate postoperative period, and thereafter, LAVI increased during the follow-up period. The SR group showed no significant difference in LAEV between the pre- and post-operative states, whereas the AF group showed a gradual decrease in LAEV during the follow-up period. In the AF group, LAEF increased immediately after the maze procedure, but thereafter returned to the preoperative level during the follow-up period. The SR group showed a gradual increase in LAEF during the follow-up period.
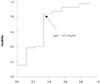
Fig. 2 shows the receiver operating characteristic (ROC) curve for the LAVI before the maze procedure. Seventy-one of 80 patients converted to SR after the maze procedure (89%). When we analyzed the area under the ROC curve for the LAVI before the maze procedure using 89% as the prevalence rate of SR conversion after the maze procedure, the area under the curve was 0.73 (p=0.03, 95% confidence interval 0.519-0.923). The sensitivity and specificity according to the LAVI cut-off level are shown in Fig. 2; the most reliable LAVI cut-off level was 117.7 mL/m2. Therefore, we proposed that a cut-off level of 117.7 mL/m2 would differentiate the conversion of AF to SR after the maze procedure in our study.
Discussion
Since its development by Cox and colleagues in 1987, the Cox maze procedure has evolved to become the gold standard for the surgical treatment of medically refractory AF.1-9) Recent reports have demonstrated a high sinus restoration rate in patients who have undergone the maze procedure to correct AF.
In agreement with previous studies,6)9) our study showed that 89% of the patients experienced restoration of SR after undergoing the maze procedure. However, according to previous studies,6)8)9)12)13) the restoration rates of both SR and atrial contraction are apparently different; SR is found in 58% to 96% of patients at 12 months after the maze procedure, whereas atrial contraction is found in 21% to 95% of patients. Additionally, the percentage of patients with restored atrial contraction after the maze procedure seems to differ with the etiology of AF.1)6)12-14)16) More than 90% of the patients with lone AF or atrial septal defects had restored atrial contraction after undergoing the maze procedure,1)6)12)16) whereas 21% to 90% of the patients with mitral valve disease had restored atrial contraction.8)13)14) Because our study was prospectively conducted on patients with mitral valve disease, we did not show a difference in restored atrial contraction rates according to the etiology of AF. Nevertheless, we found that the restoration to SR was different from the restoration of mechanical atrial function, consistent with previous studies.6)8)9)12)13)
Our study also showed that atrial mechanical function gradually increased in the SR group during follow-up, whereas atrial mechanical function decreased in the AF group. Hence, we concluded that the atrial mechanical function might be more refractory than the electrical activity after the maze procedure, in agreement with previous studies.8)17) Mechanical atrial activity might depend on the restoration and maintenance of SR, as well as on the surgical results.
According to previous studies,8)18-26) factors affecting the restoration and maintenance of SR after the maze procedure include AF duration, LA diameter, and LA size reduction. In agreement with previous studies,21-25) we found that the preoperative LAVI was an important determinant of SR restoration after the maze procedure, whereas the immediate postoperative LAVI was not associated with restoration of SR. Moreover, our study showed that preoperative LAEV and LAEF were not significantly different between the two groups. There were also no significant differences between the two groups with regard to immediate postoperative LAEV and LAEF. Therefore, we found that the preoperative LAVI was associated with the restoration of SR, whereas the immediate postoperative LAVI was not associated with the restoration of SR. We also found out that atrial mechanical function as assessed by LAEV and LAEF in the preoperative and immediate post-operative states was not associated with restoration of SR.
Our study also demonstrated that changes in LAVI, LAEV, and LAEF were different in the preoperative and postoperative states in both groups. LAVI significantly decreased in the immediate postoperative state and gradually decreased in the SR group during the follow-up period. However, in the AF group, LAVI returned to the preoperative level during the follow-up period. This may suggest the importance of the maintenance of SR in preventing re-dilation of the LA dimension. In our study, LAEV decreased gradually in the AF group after the maze procedure. Conversely, in the SR group, there was no significant change in LAEV between the pre- and post-operative states. This suggests that SR restoration may influence the differences in mechanical function between the two groups, as assessed by LAEV.
According to previous studies,8)17)18) factors affecting the restoration and maintenance of atrial contraction after the maze procedure include AF duration and LA diameter. In our study, the LAEF increased gradually in the SR group, whereas the LAEF returned to the pre-operative level in the AF group during follow-up, despite the significant increase in LAEF in the immediate postoperative states in both groups. Therefore, we believe the restoration and maintenance of SR may be important determinants of the restoration and maintenance of atrial mechanical function after the maze procedure.
We found that preoperative LAVI and reduction in atrial size may be important factors for the restoration and maintenance of SR, and the restoration and maintenance of SR may be important factors in the maintenance of restored atrial mechanical function. We concluded that the preoperative LAVI, the reduction in atrial size, and the restoration and maintenance of SR may be important determinants in the restoration and maintenance of atrial mechanical function after the maze procedure.
In our study, the ROC curve of the preoperative LAVI showed that the most reliable LAVI cut-off level for differentiating the SR group and the AF group after the maze procedure was 117.7 mL/m2. When the cut-off level of LAVI was 117.7 mL/m2, the sensitivity was 84%, and the specificity was 67%.
There are some limitations to our study. First, in spite of the prospective longitudinal nature of our study, we could not completely exclude the possibility of AF recurrence because the follow-up duration was relatively short. Second, the results may not be applicable to AF patients undergoing non-cryoablation procedures. Third, we could not completely exclude the possibility of the existence of paroxysmal AF because the patients' cardiac rhythms were followed monthly using 12-lead surface ECG or Holter monitoring. Hence, we might have failed to detect asymptomatic episodes of paroxysmal AF.
In conclusion, atrial mechanical function was successfully restored in patients whose rhythm was converted to SR after the maze procedure, irrespective of the presenting clinical characteristics and initial atrial mechanical function. The LAVI and atrial mechanical function in the immediate postoperative state did not predict the restoration and maintenance of SR. However, the preoperative LAVI successfully predicted the conversion of AF to SR. The preoperative LAVI, maintenance of atrial size reduction, and restoration and maintenance of SR may be important determinants of the restoration and maintenance of atrial mechanical function after the maze procedure.




 XML Download
XML Download