

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Subintimal angioplasty has been shown to be an effective method for the treatment of long superficial femoral artery (SFA) occlusions. In this technique, a wire is advanced across the occlusion in the subintimal space and then re-enters the true vessel lumen distal to the occlusion.1)2) One of the major factors that limit the success of this procedure is the failure of the wire to reenter the true lumen. This issue is often related to the presence of a severe calcification of the vessel wall. In this study, we present a case where an initial unsuccessful antegrade subintimal angioplasty, which was caused by a failure to re-enter the distal true lumen, was rescued by retrograde a subintimal approach through a popliteal artery.
Case
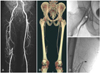
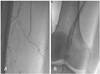
A 56-year-old man had a 12-month history of intermittent claudication after 50-meter-walking. He had a history of hypertension, diabetes mellitus, and smoking.The physical examination showed a good femoral pulse; however, the right popliteal and dorsalis pedis pulses were not palpable. The right ankle-brachial index (ABI) at rest was 0.3. Computed tomography and conventional angiography showed that this patient had a total occlusion in the right SFA, that was 230 mm in length and started in the ostium and continued to the distal level (Fig. 1). The popliteal artery was reconstituted via collaterals and was normal in caliber. The left common femoral artery (CFA) was punctured and a 7 Fr Balkin sheath (Cook, Bloomington, IN, USA) was moved into the right external iliac artery. An angled 0.035 inch hydrophilic guidewire (Radifocus; Terumo, Tokyo, Japan) with the support of a 5 Fr catheter (Glidecath; Terumo, Tokyo, Japan) were used to create a subintimal dissection plane above the level of the occlusion. After the successful formation of the subintimal dissection and wire loop, the wire was moved through the subintimal space down to the distal occlusion site with the support of the Glide catheter (Fig. 2A). An attempt was then made to pass the wire into the distal true lumen. However, reentering the wire into the true lumen distal to the occlusion was impossible (Fig. 2B). Since the popliteal artery distal to the occlusion site was diseasefree and normal in caliber, a retrograde approach through the popliteal artery was planned as an alternative. On the next day, an ultrasound-guided ipsilateral retrograde popliteal artery puncture was carried out. Using diagnostic angiograms and bony landmarks, a puncture point was chosen by fluoroscopy, which was above the knee but 6cm below the distal tip of the occlusion. With the patient in the prone position, a probe was used to visualize the popliteal artery. The probe was then tilted at an appropriate angle in the transverse plane to avoid superimposition of the vein and then slightly angled in the craniocaudal direction such that the entry point would be in-plane and the tip of the needle would be seen entering the popliteal artery. The artery was then punctured with a simple Seldinger needle using the single-wall technique, and a 6 Fr sheath was introduced near the distal occlusion site (Fig. 3A). The left CFA was then punctured in the supine position and a 7 Fr Balkin sheath was moved into the right external iliac artery. Thereafter, a attempt was made to pass the guide wire in a retrograde fashion. However, passage of the wire into the subintimal space across the distal occlusion site through this process was very difficult and was barely achieved by forcefully pushing a 6 Fr sheath-introducer (Terumo, Tokyo, Japan) against the distal occlusion cap. An angled 0.035 inch hydrophilic guidewire (Radifocus; Terumo, Tokyo, Japan) with the support of the 5 Fr catheter (Glidecath; Terumo, Tokyo, Japan) was then moved through the subintimal space in a retrograde fashion. The retrograde wire was successfully passed into the true lumen of the right CFA (Fig. 3B), and attempt was then made to pass the retrograde wire into the Balkin sheath, which was placed in the right external iliac artery. After the wire entered the Balkin sheath without difficulty (Fig. 3C), it was guided outside the body and a subsequent procedure was performed along the "flossing"-type guide wire in the antegrade direction. After dilatation with a 5.0×80 mm balloon (Powerflex, Cordis, Miami, FL, USA), three self-expandable nitinol stents (Smart 6.0×100 mm, Smart 7.0×100 mm, and Smart 8.0×59 mm; Cordis, Miami, FL, USA) were placed along the SFA from the distal to proximal including the ostium, which yieldied a satisfactory final result (Fig. 3D). The patient was discharged uneventfully 6 days after the procedure and remained clinically stable during the 7 months of clinical follow up.
Discussion
Since Bolia introduced subintimal angioplasty,1) this technique has been widely used in the treatment of femoropopliteal occlusions and has providied a high procedural success rate with an acceptable long-term outcome, especially in high surgical risk groups.3) In this technique, a wire is intentionally moved across the occlusion in the subintimal space and exits back into the true vessel lumen distal to the occlusion. The presence of at least a 5 mm stump at the origin of the SFA is required to increase the success rate of this technique.2)4) Unless the patient has an adequate stump, the success rate usually decreases.4) However, the most common cause of failure for subintimal angioplasty is the inability to re-enter the true lumen distal to an occlusion, which has an incidence of 13-26%.5) To overcome the re-entry failure, distal re-entry devices, such as the intravascular ultrasound (IVUS)-guided CrossPoint TransAccess catheter (Trans-Vascular, Menlo Park, CA, USA) or Outback catheter (Perclose, CA, USA), were developed and shown to be feasible.5)6) In this case, after failure to reenter the distal true lumen, other maneuvers should be required. Since reentry devices were not available in our country and the popliteal artery was normal in caliber and disease-free, we decided to perform a retrograde approach via the popliteal artery. Retrograde popliteal artery puncture has not been very popular for the treatment of SFA lesions. Possible complications in this technique include popliteal artery occlusion at the puncture site, distal emboli, and arteriovenous fistula due to unintentional puncture of the popliteal vein.7) Thus, to avoid these complications, an ultrasound guided approach is needed. The ultrasound approach allows for the visualization of atheromas in the popliteal artery, prevent a popliteal aneurysm, and help to avoid puncturing the popliteal vein.7) In our case, the ultrasound could see the tip of the Seldinger needle entering the popliteal artery and the puncture was successfully made during the first attempt. Therefore, we believe that ultrasound guidance greatly facilitates the puncture of the popliteal artery. After the retrograde wire is passed into the proximal true lumen, it can be maneuvered into the antegrade sheath or catheter. If the wire cannot enter the antegrade sheath or catheter, a loop snare can be used to capture the retrograde wire. When the retrograde wire is guided outside the body, creating a "flossing"- type guide wire, antegrade angioplasty using a bigger size balloon or stent can be stably done. In addition, antegrade angioplasty can eliminate the need for large sized retrograde sheaths or catheterization of distal arteries; thereby, limiting the trauma to distal vessels. This case suggests that the retrograde subintimal angioplasty is a safe and feasible method for the treatment of long SFA occlusions. However, due to the technical complexity and the possibility of unusual complications related to a potential popliteal puncture, it may be reasonable to reserve this method as a final option in the treatment of SFA occlusion.

 XML Download
XML Download