

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background and Objectives
Pressure monitoring and injection of contrast media after piercing the fossa ovalis are used to avoid life-threatening complications during transseptal procedures. However, when performing those maneuvers, the information provided can only be obtained after having pierced structures that may not have been the intended target. When we injected the contrast media through a Brockenbrough needle before piercing the fossa, the dye that had collected under the membranous septum tented by the transseptal equipment (tenting) was observed on the left anterior oblique (LAO) projection and this indicated the fossa ovalis. This study was performed to evaluate the usefulness and safety of tenting in order to identify the membranous septum during transseptal procedures.
Subjects and Methods
Contrast injections were performed on the fossa ovalis and the septal wall surrounding it during 64 transseptal procedures. The rates of dye staining and tenting in both the muscular and membranous septums were compared.
Results
No areas of the muscular septum exhibited any tenting. Various rates of dye staining of those areas were observed. However, the membrane of the fossa exhibited tenting without dye staining in all 64 cases. The sensitivity of the tenting without dye staining to identify the Fossa was 98%, and the specificity was 100%.
Figures and Tables
Fig. 1
Angiographic images before and after the interatrial septal puncture. A: TENTING (arrows): a sharp conical collection of dye around the tip of the transseptal puncture system in the left anterior oblique projection (LAO 40°), indicating the membrane of the fossa ovalis. B: piercing with the brockenbrough needle: contrast media (arrow) is injected into the left atrium.
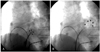
Fig. 2
Various TENTINGs (arrows) in the left anterior oblique projection (LAO 40°). Every TENTINGs exhibit sharp edges as arrow heads. TENTING: a sharp cornical collection of dye around the tip of the transseptal puncture system.

Fig. 3
Dye staining. A: the left anterior oblique projection (LAO 40°) shows a blunt dye staining (arrows) around the tip of transseptal puncture system directed toward the muscular septum located superior to the fossa ovalis. B: after directing the fossa correctly with the puncture apparatus, the right anterior oblique projections (RAO 40°) was examined. The dye staining just above the tip of the puncture system sustained for a long period.

Fig. 4
A dye collection mimicking TENTING. A: the left anterior oblique projection (LAO 40°). Dye collections under the septal wall other than fossa are seen sometimes but are not sharp as that of TENTING (arrows). B: continuous injection of contrast media at the very point resulted in dye staining (arrows), which sustained for several minutes. TENTING: a sharp cornical collection of dye around the tip of the transseptal puncture system.

Fig. 5
The transseptal puncture system lying against the roof of the middle portion of the coronary sinus. A: leftward shifting during TENTING mimics the membrane of the fossa (arrow). B: a dye injection after advancing the Brockenbrough needle reveals localized extravasation of the contrast media (arrow). TENTING: a sharp cornical collection of dye around the tip of the transseptal puncture system.
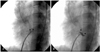
Fig. 6
Right anterior oblique projections (RAO 40°) achieved just after testing TENTING with transseptal puncture system (TSPS) in LAO projections. The tips of the TSPSs are parallel to the CS catheters and locate between the CS catheters and the anterior aspect of the vertebral column which indicate the posterior wall of the left atrium. Usually, the level of the tip of the TCPS on the septum is below that of the His catheter, which indicates the lower margin of aortic root (A). The level of the tip is above that of the His catheter in B. These situations are usually observed in the cases exhibiting more vertical hearts in RAO projections. hRA: high right atrium, CS: coronary sinus, RVa: right ventricular apex.


Table 2
Tenting and dye staining in the areas around the fossa ovalis

Tenting: the dye that had collected under the membranous septum tented by the transseptal equipment. Dye staining tests were performed on the septum around the fossa. Two areas were tested in one patient until 30 tests in each area were enrolled. Incidental dye testing against the CS roof in one patient showed tenting without dye staining. CS: coronary sinus.
References
1. De Ponti R, Cappato R, Curnis A, et al. Trans-septal catheterization in the electrophysiology laboratory: data from a multicenter survey spanning 12 years. J Am Coll Cardiol. 2006. 47:1037–1042.
2. Cope C. Technique for transseptal catheterization of the left atrium: preliminary report. J Thorac Surg. 1959. 37:482–486.
3. Ross J Jr, Braunwald E, Morrow AG. Transseptal left atrial puncture: new technique for the measurement of left atrial pressure in man. Am J Cardiol. 1959. 3:653–655.
4. Ross J Jr, Braunwald E, Morrow AG. Left heart catheterization by the transseptal route: a description of the technique and its applications. Circulation. 1960. 22:927–934.
5. Brockenbrough EC, Braunwald E. New technique for left ventricular angiocardiography and transseptal left heart catheterization. Am J Cardiol. 1960. 6:1062–1064.
6. Brokenbrough EC, Braunwald E, Ross J Jr. Transseptal left heart catheterization: a review of 450 studies and description of an improved technique. Circulation. 1962. 25:15–21.
7. Shaw TR. Anterior staircase manoeuvre for atrial transseptal puncture. Br Heart J. 1994. 71:297–301.
8. Inoue K. Percutaneous transvenous mitral commissurotomy using the Inoue balloon. Eur Heart J. 1991. 12:B. 99–108.
9. Yoon JH, Park KS, Choi KH, Hwang SO. Percutaneous balloon mitral valvuloplasty in patient with mitral stenosis and kyphoscoliosis. Korean Circ J. 1993. 23:320–324.
10. Shin YJ, Shim WH, Yoon YS, Chung NS. Percutaneous balloon mitral valvuloplasty in pregnancy. Korean Circ J. 1992. 22:858–862.
11. Ballal RS, Mahan EF 3rd, Nanda NC, Dean LS. Utility of transesophageal echocardiography in interatrial septal puncture during percutaneous mitral balloon commissurotomy. Am J Cardiol. 1990. 66:230–232.
12. Hung JS, Fu M, Yeh KH, Chua S, Wu JJ, Chen YC. Usefulness of intracardiac echocardiography in transseptal puncture during percutaneous transvenous mitral commissurotomy. Am J Cardiol. 1993. 72:853–854.
13. Park SH, Kim MA, Hyon MS. Percutaneous balloon mitral valvuloplasty guided by transesophageal echocardiography. Korean Circ J. 1997. 27:744–757.
 XML Download
XML Download