

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Mesenchymal stem cell (MSC) or progenitor cell transplantation has the potential to improve ventricular function, especially if it is administered during the acute stage of myocardial infarction.1-3) In addition, another potential benefit of MSCs is that MSCs may not provoke immune rejection.4-6) However, the safety of MSC transplantation has not yet been clearly established. It has been reported that transplanted MSCs led to poor cell to cell coupling with recipient cardiac cells and promoted potential proarrhythmia.7) But in other studies MSCs were shown to repair conduction blocks8) and express gap junctions.9) Pak et al.10) previously reported that MSC transplantation induces cardiac nerve sprouting in a swine model of myocardial infarction (MI). Cardiac sympathetic hyperinnervation may improve ventricular function. However, it has also been shown to induce lethal arrhythmias.11)12) Based on these studies, we hypothesized that human MSC (hMSC) transplantation may result in sympathetic hyperinnervation, impaired conduction, and ventricular tachyarrhythmias. Therefore, the purpose of this study was to determine the risk of ventricular tachyarrhythmias after hMSC transplantation in a canine model. We also sought to determine how hMSC transplantation affects messenger ribonucleic acid (mRNA) expression of the nerve growth factor (NGF) and connexin (Cx) 43, cardiac sympathetic hyperinnervation, and gap junctional expression.
Materials and Methods
The protocol used in this study was approved by the Institutional Review Board and the Institutional Animal Care and Use Committee of Anam Hospital of Korea University and conformed to the guidelines of the American Heart Association on human and animal studies.
Preparation of human mesenchymal stem cell
Human bone marrow, which was used for subsequent transplantation, was harvested from the posterior iliac crest of healthy volunteers. The concentration of nucleated cells in the bone marrow aspirates was 26.7± 2.4 million cells per milliliter. Mononuclear cells were separated from red cells by density gradient centrifugation using Ficoll Paque (density 1.077 g/cm3, American Pharmacia Biotech, Piscataway, NJ, USA). The buffy coat was collected and washed twice by centrifugation at 1,500 rpm for 5 minutes. The cell pellet was re-suspended in culture media at 37℃ and 5% CO2. Cells were initially plated in 25 cm2 vented culture flasks (Costar, Cambridge, MA, USA) at 2×106 cells per milliliter. After 3 days, the media and non-adherent cells were discarded. Cultures were fed biweekly until the flask cultures were confluent. Fibroblast-like cells started forming 4 days after cell culture. Adherent cells were passed three times to eliminate hematopoietic stem cells, and were then progressively expanded to 10 stack cell factories (Nalgene Nunc International, Napervile, IL, USA). The cultured cells were characterized as human mesenchymal stem cells (hMSC) by flow-cytometry (CD29+, CD44+, CD90+, CD105+, CD31-, 34-, and CD45-) and quantitative Reverse Transcription Polymerase chain Reaction (qRTPCR) (Oct-4 gene expression). Prior to epicardial injection, adherent cells were trypsinized, washed and re-suspended.
Surgical preparation
A total of 11 mongrel dogs (body weight 28-35 kg) were used. We implanted an implantable defibrillator (ICD: Model 7275 VVED-DDDR, Medtronic Inc.) in all dogs using the left internal jugular transvenous approach. An ICD coil electrode was positioned on the right ventricular apex endocardially (Fig. 1A). The ICD generator was implanted in the lateral chest after closing the pericardium. The measured defibrillation threshold in 5 dogs was 15.2±5.3 J. The ventricular fibrillation (VF) was detected when the ventricular rate exceeded 210 bpm. The ICD was followed up at 24 hours, 1 week, and 2 weeks after surgery and kept in the monitoring mode.
Human mesenchymal stem cell transplantation and endocardial mapping
We selected 5 sites for hMSC injections on the left ventricular (LV) mid anterior wall in the area between the left anterior descending coronary artery and the left circumflex coronary artery. We marked 5 evenly separated sites that spanned a 30 mm diameter circle with suture materials, and hMSCs (1×107 cells in 1 mL) were injected epicardially at these sites (0.2 mL in each point; Fig. 1B). In the Sham animals, culture media of the same volume as the hMSC was injected. The pericardium was then loosely closed. Dogs that survived more than 4 weeks were sacrificed 32.1±5.7 days after the first surgery. The tissues were then harvested for immunohistochemical and mRNA analyses. One dog in hMSC group died suddenly; therefore, its cardiac tissue was not included in the histological and mRNA analyses due to the time delay before necropsy.
The documented arrhythmic events in ICD were manually analyzed. 3-dimensional isochronal maps were generated by LV endocardial contact bipolar mapping (70-100 points, during high right atrial pacing, pacing cycle length 500 ms) using a NavX system (St. Jude Medical Inc. Minnetonka, MN, USA) in 2 animals injected with hMSC before sacrifice.
Immunohistochemical sudies
Hearts were fixed with 4% formalin. They were then sampled, paraffin embedded and processed routinely for immunohistological examinations.11) We performed tyrosine hydroxylase (TH) staining to detect sympathetic nerves, Cx43 immunostaining to detect gap junctions, and human nucleolin (hNC) staining to detect hMSC. 5 µm thick transmural sections that were formalinfixed and paraffin embedded were stained for TH, Cx43, and hNC using a modified immunocytochemical AB complex method as described previously.10) Primary antibody concentrations were 1 : 200 for TH (Abcam Inc., Cambridge, UK), 1 : 100 for Cx43 (Chemicon International Inc., USA.), and 1 : 400 for hNC (Abcam Inc., Cambridge, UK), respectively. The immunoreactive products were visualized by incubating the tissue sections in a DAKO Liquid DAB Substrate Chromogen system (Dako, Copenhegen, Denmark) and counterstained with diluted hematoxylin.
Messenger ribonucleic acid analyses for nerve growth factor-β
mRNA expression of NGF-β and Cx43 was quantified using qRT-PCR with a Perkin-Elmer ABI Prism 7,700 sequence detection system. qRT-PCR was performed with a AmpliTaq Gold polymerase (Perkin-Elmer ABI) and 20 ng of cDNA per reaction (Taqman Gene Expression Assays, Applied Biosystem Inc.).13) The cycle threshold (Ct) values for 18s rRNA and the mRNA of interest were compared and calculated using sequence detector software (Perkin Elmer ABI). Relative transcript levels were calculated as χ=2_△△Ct where ΔΔCt=ΔE-ΔC and ΔE=Ct experimental-Ct 18s rRNA; ΔC=Ct control-Ct 18s rRNA. For comparison, the Ct-value of the sham group was used as the normal control.
Data analyses
TH slides were evaluated for nerve density. The entire slide was scanned with a 100× objective and 4 microscopic fields with the highest intra-myocardial nerve densities at the right upper, right lower, left upper and left lower quadrants of each slide were selected. In each of the four fields, the cardiac nerves were identified as THimmunostaining-positive fibrillar structures, between myocardial cells, when they were longer than 10 µm and stained brown (RGB values: Red 22-125, Green 4-77, and Blue 4-55). In addition, the digital images at 400× magnification were saved. The gap junctions located on the cell membranes of each myocardial cell were identified by Cx43-immunostaining-positive linear structures. To evaluate the density of the gap junctions, we obtained 4 digital pictures at each quadrant of the tissue slide at 400× magnification. The percent area of the nerve cells and gap junctions {DAB responsive area/the area of digital image (1.41 µm2)×100 (%)} were calculated from the immuno-staining using Image Pro software (MediaCybernetics Inc.) by a single investigator who was blinded to the groups.14) The density of the cardiac sympathetic nerve or gap junctions were calculated by dividing the nerve or gap junction areas by the total area examined (% area), respectively. All values were expressed as mean±SD. Between-group comparison was carried out with student's t-test for the continuous variables, and Fisher's exact test for the non-continuous variables. Statistical significance was defined as a p<0.05.
Results
Documented ventricular fibrillation after human mesenchymal stem cell transplantation
Table 1 summarizes the incidences of VF and sudden cardiac death (SCD). Among the 6 animals transplanted with hMSC, one dog died suddenly 6 days after surgery. The ICD recorded VF at the time of the SCD episodes. In the necropsy, no other cardiovascular reasons for SCD other than VF were found. We programmed the ICD to the monitor mode to only prevent shock delivery. This allowed us to determine if some VF episodes could spontaneously terminate without shocks. In the hMSC group another dog also manifested non-sustained VF; however this dog did not die suddenly (Fig. 1C). The ICD electrograms revealed spontaneous VF in 2 of the 6 dogs (33.3%). In comparison, no VF or SCD episodes were documented in the sham control group (0/5; 0%).
Engraftment of human mesenchymal stem cell without immune rejection
For the immunohistochemical analyses, hNC positive hMSC were observed in the myocardium 4 weeks after injection (Fig. 2A). As a result of inflammation after surgery there were some polymorphonuclear cells at the injection sites. However, there was no evidence of lymphocytic infiltration or immune rejection (Fig. 2B). The survival rate of hMSC was approximately 3%, 4 weeks after myocardial injection.
Human mesenchymal stem cell transplantation increases nerve growth factor-β mRNA expression and cardiac sympathetic nerve sprouting
qRT-PCR for mRNA expression of NGF-β was performed on tissue removed from the area of the hMSC injection. NGF-β mRNA expression in the hMSC group was 56.0±66.8 (p<0.01) fold higher than in the Sham group (Fig. 3A). TH-positive sympathetic cardiac nerve densities in the areas of hMSC injection were determined from 320 digital images at areas of highest cardiac nerve density in 20 slides. Fig. 3C and D show the distributions of TH-positive cardiac sympathetic nerves in each group. Hearts from the hMSC group showed very high sympathetic nerve densities. There were actively arborizing large nerves and TH positive ganglia. By contrast, dogs in the sham control group rarely had TH positive sympathetic nerve twigs. The calculated % areas of the cardiac sympathetic nerves in the tissue of hMSC group (0.51±0.40%) was significantly higher than those of the Sham group (0.15±0.13%, p<0.03; Fig. 3B).
Human mesenchymal stem cell transplantation reduces Cx43 mRNA expression and gap junctions
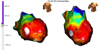
qRT-PCR for mRNA expression of Cx43 was performed on tissue removed from the area of hMSC or vehicle injection. Cx43 expression in the hMSC group was 0.59±0.29 fold lower than that of the Sham group (p<0.001, Fig. 4A). After quantification of gap junctions from 320 digital images in 20 slides stained with Cx43 immunostaining the density of gap junction was found to be lower in hMSC group compared with the Sham control group (Fig. 4C and D). The % area of Cx43 positive gap junctions in hMSC group was significantly lower than that of the Sham group, which was consistent with the Cx43 mRNA expression (1.64±0.79% vs. 2.12±1.07%. p<0.001; Fig. 4B). Fig. 5 displays the remarkable conduction delay the we observed at the hMSC transplantation area in the isochronal map of LV endocardial contact mapping.
Discussion
In this study, we successfully transplanted and engrafted hMSC in a canine model without any immune rejection. However, the hMSC transplantation did increase NGF-β expression and cardiac sympathetic hyperinnervation, and reduced the expression of Cx43 mRNA and gap junction density. In addition, VF and SCD, which are associated with potential proarrhythmia, were encountered in this model after hMSC transplantation.
Human mesenchymal stem cell transplantation: potential for treatment of heart failure
Cellular transplantation is an emerging new technology that can be potentially used for the treatment of heart failure. MSCs have several merits compared with other cell sources in relation to cardiac cell therapy, including no ethical problems, better cellular coupling with recipient cells compared to skeletal myoblast,8)15) and immunological privilege.4-6)16) In addition, the immunologically privileged status of MSCs may extend to xenograft settings.17) Several clinical trials have shown that the use of hMSC precursors were effective in managing heart failure especially if used during the acute stage of myocardial infarction.1)2)18-20) However, the improvement of LV function has been shown to be minimal and may not be long lasting,21) and the mechanism of action is still unknown.
Electrophysiologic limitations of human mesenchymal stem cell transplantation
Menasche et al.22) reported that 4 out of 10 patients with ischemic cardiomyopathy, who received transplanted autologous skeletal myoblasts, experienced late sustained VT. These findings suggest that cellular transplantation has the potential to develop into cardiac arrhythmia. The observed arrhythmias may be due to the lack of gap junctions expressed in transplanted skeletal myoblasts, which results in large excitable gaps in the recipient heart and aberrant electrical activity.23) Although Beeres et al.8) demonstrated that MSCs express gap junctions with sufficient coupling. Since the cells are not excitable, they will be unable to carry the action potential over larger distances and will be unlikely to support contractility due to the absence of a well-developed functional contractile apparatus. Chang et al.7) also reported potential arrhythmia in an optical mapping study of co-cultured MSC and ventricular myocytes. This occurred as a result of reduced conduction velocity, which was due to increased tissue heterogeneity. This was observed despite the presence of functional gap junctions that involved MSCs. Consistent with previous studies, we observed a reduction in both gap junctional expression and the conduction velocity at the sites of hMSC transplantation. Even though gap junctions exist, poor differentiation to functional cardiomyocyte or insufficient ion channel expression may induce conduction delay, localized reentry, and proarrhythmia.
Several recent clinical trials showed that intracoronary injection of bone marrow derived stem cells resulted in no proarrhythmia in humans.1)2)18-20) However, endothelial progenitor cells were used in these studies, and the average LV ejection fractions was relatively high (41.0 to 48.9%), indicating that the enrolled patients did not all have significant LV dysfunction. Therefore, these studies do not rule out the possibility of stem cell proarrhythmia in hearts with more severe organic diseases. Compared with previous clinical studies that have used intra-coronary infusion of bone-marrow-derived cells, our model produced a high density of hMSC that were localized within 3 cm around the pacing electrode. The localized high density hMSC may have exacerbated the problems of cell to cell conduction and proarrhythmia.24) However, intra-coronary infusion of hMSC is not feasible due to the large size of hMSC and the risk of coronary embolism.
Mesenchymal stem cell induced cardiac sympathetic nerve sprouting and sudden death
There are three possible cellular mechanisms by which MSCs contributed to the restorative action and improvement of ventricular function. The first potential mechanism is that the MSCs differentiate into functioning cardiac structures such as cardiomyocytes,25-31) vessels,26)28) fibroblasts,25)26) or nerve.32) The second is that the MSCs change their function by fusing with recipient cells.33)34) Finally the third potential mechanism is that stem cells induce angiogenesis or sympathetic nerve sprouting by paracrine action.35)
Sympathetic nerve sprouting, and its heterogeneity, is a known substrate for lethal ventricular arrhythmias.11-13) Sympathetic nerve activation exerts significant effects on electrophysiologic properties such as automaticity, triggered activity, refractoriness, and conduction velocity of myocardial cells.36)37) Although we have previously reported that enhanced nerve sprouting occurs in a MSC transplanted swine model,10) sympathetic hyper-innervation and its mechanism were not proven at that time. In this study, we documented the elevation of NGF-β expression and sympathetic hyperinnervation in a canine model of transplanted hMSC.
Study limitations
There were multiple other factors that could have been responsible for VF in hMSC transplanted hearts that were independent of sympathetic hyperinnervation or reduced gap junction. However, sympathetic hyperinnervation and reduced gap junctions after hMSC transplantation with EpiP are novel findings, and might be contributing factors that cause VF. Although a pathologist determined no evidence of immune rejection, we cannot absolutely exclude undetected proarrhythmic effects from the cellular xenograft. We did not perform long-term monitoring of the experimental animals.





 XML Download
XML Download