

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Hypertension is an important worldwide public-health problem because of its high frequency and the concomitant risk of cardiovascular and kidney disease.1) This condition has effected approximately one forth of the world's population2) and it has been identified as the leading risk factor for mortality. Hypertension is influenced by the interaction of various environmental and genetic factors. The genetic contribution is speculated to make up about 30% to 40% of the variation of blood pressure.3) Through its modulation of salt and water homeostasis, the renin-angiotensin system (RAS) is a major regulator of blood pressure.4) Since RAS is a well known pathophysiologic pathway that's involved in BP regulation, the genes that encode the components of RAS have been suggested to be promising candidate genes for hypertension.5)
In the RAS cascade, angiotensin is cleaved by renin to produce angiotensin I, which is further converted to angiotensin II through the action of angiotensin I converting enzyme (ACE).6) Angiotensin II binds to several types of receptors. Two of these are coupled with the G protein system.7) The type 1 receptor mediates vasoconstriction and the proliferative action of angiotensin II, while the type 2 receptor inhibits cell proliferation and mediates apoptosis.7) The cellular effects of angiotensin II in adult humans are mainly mediated by the angiotensin type 1 receptor. The angiotensin II receptor type 1 (AGTR 1) gene has been cloned and mapped to the long arm of human chromosome 3 (3q21-q25).8) The polymorphism resulting from adenosine to cytosine transversion at position +1166 in the 3' untranslated region of the gene has been the subject of many research studies.9)10)
Currently, we are still far away from understanding the genetic background of hypertension. The aim of this study was to determine the associations of the AGTR 1 A1166C marker with essential hypertension and cardiovascular diseases in Korean adolescents, We also wanted to evaluate the AGTR 1 A1166C in terms of its application as a genetic marker for the susceptibility to hypertension and cardiovascular diseases.
Subjects and Methods
Patients
Forty hypertensive patients were involved in this study. The participants' ages ranged from 16 to 17. Their systolic blood pressure was greater than 145 mmHg or their diastolic blood pressure was greater than 90 mmHg, which was over the 95th percentile for both sexes according to the normal blood pressure range reported by Hong et al.11)
The hypertensive adolescents were boys and girls from middle and high school and who were selected during routine health check ups. All the subjects gave written informed consent for participation in this study.
Clinical features
All the hypertensive students were sent to our pediatric clinic. Their elevated blood pressure was confirmed by averaging the three blood pressure measurements that were taken after 5 minutes of rest using an oscillometric monitor. The study subjects had never been diagnosed or treated for hypertension before. Their height and body weight were measured. The body mass index (BMI) and obesity index (OI) were calculated from the measurements. The BMI was defined as weight (kg) divided by height squared (m2). The OI was calculated by the following equation using the standard weight as the value corresponding to the 50th percentile of weight measurement charts of Korean children and adolescents.
Obesity index (%)=(weight measured-standard weight)/standard weight×100
Obesity was defined as an OI above 120 percent. Triceps and subscapular skin fold thicknesses were determined using a skin fold Lange caliper. The mid-upper arm circumference was measured in centimeters. Fat mass and fat distribution were measured by bioelectrical impedance analysis (Inbody 3.0, Biospace, Seoul, Korea).
Intima-media thickness of the common carotid artery
Measurements of the carotid artery were made using a real-time B-mode ultrasound imager (iU22, intelligent Ultrasound System; Philips, Amsterdam, Netherlands) and a 12.5 MHz probe. For all subjects, the intima-media thickness (IMT) and lumen diameter were measured in the same carotid arterial segment by the same radiologist. The patients were in the supine position for 30 minutes before the measurements were made. The following equations were used to calculate the carotid artery compliance and elasticity.
Intimal medial thickness (IMT, mm)
Systolic diameter (sD, mm)
Diastolic diameter (dD, mm)
ΔP: pulse pressure
Lumen cross-sectional area=πdD2/4
Wall cross-sectional area=π(dD/2+IMT)2-π(dD/2)2
Cross-sectional compliance={π(sD2-dD2)}/4ΔP (mm2.mmHg-1)
Cross-sectional distensibility=(sD2-dD2)/(dD2ΔP) (mmHg-1.10-2)
Pulse wave velocity and the ankle brachial index
The brachial-ankle pulse wave velocity (BaPWV) and ankle brachial index (ABI), were measured by a VP-1000 (Colin Co., Komaki, Japan). Using the volume plethysmographic technique, the PWV and ABI (the ratio of the systolic blood pressure in the ankle to that in the brachial artery), the blood pressure of the extremities, the electrocardiography and the heart sounds were obtained simultaneously.
The cuffs were wrapped on both the arms and ankles, and electrocardiogram electrodes were placed on the left sternal border. The cuffs automatically inflated and deflated as the pulse wave contours in the four extremities were recorded. The cuffs were attached to the plethysmographic sensor, which determined the volume pulse form.
The blood pressure was measured from the oscillometric pressure sensor. The BaPWV was determined by the pulse transit time and the distance between these two segments. The distance of each segment was calculated automatically, based on the height of the subjects. All the measurements were done during regular sinus rhythm.
Aldosterone, renin, insulin, angiotensin converting enzyme, homocysteine, vitamin B12 and folate
Venous blood was drawn from all the patients after they fasted overnight. The samples were kept at -70℃ for subsequent assay. The serum concentrations of aldosterone, renin, insulin, vitamin B12 and folate were evaluated by radioimmuno assay (RIA) using a COBRA-II Gamma Counter (Packard, California, USA). The ACE concentration was measured via the ELISA method using a COBAS MIRA (Roche, Switzland). The homocysteine level was measured by chemilumino immunoassay (CLIA) using an ADVIA Centaur HCY (Bayer, USA).
Determination of the angiotensin II receptor type 1 A1166C genotype
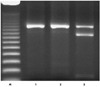
To determine the angiotensin II type 1 receptor genotype, genomic DNA was extracted from whole blood using a QIAamp DNA Blood mini kit (Qiagen, Valencia, CA, USA). The polymerase chain reaction (PCR) process involved 5 minutes of denaturation in 94℃, followed by 30 cycles of 1 minute denaturation in 94℃, I minute in 55℃ and 1 minute in 72℃ with the primers 5'-GCA CCA TGT TTT GAG GTT-3' and 5'-CGA CTA CTG CTT AGC ATA-3' (Table 1). This resulted in a 527 bp PCR product (from the non-transcribed 3' region of the gene). Upon cleavage with 14 U of restriction enzyme DdeI (New England Biolab, Bererly, MA) and after being electrophoresed on 2% agarose, the allele C produced two bands at 417 and 110 bp, while the A allele remained undigested (Fig. 1). The purified PCR products were sequenced using an ABI3100 genetic analyzer (Applied Biosystems).
Statistical analysis
All statistical analyses were performed with the use of the Statistical Package for Social Science (SPSS)/PC software package (SPSS version 11.0) program. Descriptive statistics are presented as means and standard deviations.
The correlations among the continuous variables were determined with using t-tests. A p less than 0.05 was considered as statistically significant.
Results
40 subjects participated in the present study. 35 of them had the AA genotype (87.5%) and 5 had the adenylate cyclase (AC) genotype (12.5%) (Table 2).
There were no significant differences in the anthropometric data such as height, weight, BMI, OI, skinfold thickness, arm circumference, fat mass and fat distribution between the AA genotype and the AC genotype (Table 3). Table 4 illustrated the comparison of blood pressure according to the AGTR 1 genotype. Neither the systolic nor diastolic blood pressure showed statistically significant differences according to a certain genotype (Table 4).
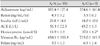
The serum aldosterone, renin, insulin, ACE, vitamin B12 and folate levels did not display any association with genetic polymorphism. The serum homocysteine level was significantly higher for the AC genotype than for the AA genotype (11.9±2.9 umol/L vs 17.1±4.2 umol/L, p<0.05) (Table 5).
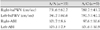
The carotid IMT was 5.0±0.1 mm in subjects with the AA genotype and this was 8.0±0.2 mm in the subjects with the AC genotype. The AC genotype was significantly associated with a larger carotid IMT. The systolic diameter and diastolic diameter tended to be slightly larger in the subjects with the AA homozygocity than in the subjects with the AC genotype, but this was without statistical significance. Cross sectional compliance and cross sectional distensibility did not show any statistical difference between the two groups (Table 6).
There were no significant differences in the PWV and ABI among the two groups (Table 7).
Discussion
Even though much progress has been achieved during the past twenty years concerning our knowledge of the genetic background of essential hypertension, the studies that have been done on the candidate genes among different populations have shown inconsistent and often unclear results. Jung et al.12) published in 2005 that no relevance was found between the β2-adrenergic receptor gene and hypertension in the Korean population.
The RAS plays a central role in salt and water homeostasis and the maintenance of vascular tone and cardiovascular structure, and thus, in the regulation of blood pressure.7) Renin is released from the kidney into the blood in response to decreased renal perfusion pressure.13) Circulating renin then cleaves angiotensinogen to the inactive peptide angiotensin I.14) Angiotensin I, in turn, converts into the active octapeptide angiotensin II by the action of angiotensin converting enzyme.15) Angiotensin interacts with at least two receptor subtypes, AGTR 1 and AGTR 2.16) Many of the deleterious effects of angiotensin II are thought to be mediated through interaction with AGTR 1.13) Binding to AGTR 1 leads to vasoconstriction, release of aldosterone and retention of salt and water.15) The genomic effects of AGTR 1 activation seem to be the result of the intracellular activation of transcription factors such as nuclear factor kB and activator protein 1.15)
The genes that encode the RAS are thought to participate in the pathogenesis of essential hypertension. AGTR 1 has been extensively studied and its involvement in the development of hypertension has been analyzed by linkage and association studies in numerous populations. Despite all the efforts, the role of the AGTR 1 gene locus still remains controversial. In a study conducted by Stankovic et al.,16) the CC genotype influenced the risk of essential hypertension in a gender-specific manner in the Serbian population.
Zhu et al.17) reported in their study which involved 150 subjects that the AGTR 1 A1166C polymorphism is associated with essential hypertension and carotid atherosclerosis in the Chinese population. In another study conducted by Rehman et al.18) the A1166C polymorphism had no association with blood pressure, but it may have an influence on the aortic PWV in Malays. Miyama et al.19) also published a recent report that AGTR 1 gene polymorphism does not influence the onset of essential hypertension.
In the present study, no differences in the anthropometric data and blood pressure were observed between the AA genotype and the AC genotype of the AGTR 1 gene. The homocysteine level was significantly higher in the subjects with the AC genotype than that in the subjects with the AA genotype. Mild hyperhomocysteinemia, defined on the basis of plasma concentration ranging between 16 and 30 umol/L, is independently associated with the development of coronary disease, cerebral and peripheral vascular disease and deep-vein thrombosis in the general population.20)
In the present study, the carotid IMT in the group with the AC genotype was significantly larger than that of the AA genotype group. An increased IMT is associated with vascular risk factors and the development of advanced atherosclerosis, which includes coronary artery diseases.21-24) In a study conducted by Hong et al.,25) the serum homocysteine level was significantly increased in hypertensive adolescents. Sharma et al.26) reported that hyperhomocysteinemia initiates atherosclerosis by modulating cholesterol biosynthesis and by significantly increasing the level of other cardiovascular risk factors and markers. Dai et al.27) reported in their research that an increased homocysteine level leads to atherosclerosis by an immunoregulatory mechanism. We speculated that the rise in the homocysteine level led to the increase in the carotid IMT (cIMT) in our study. These findings collectively suggest that the AC genotype may be a risk factor for the development of atherosclerosis and coronary heart disease.
Sen et al.28) demonstrated for the first time in 2007 that AGTR 1 contributes to homocysteine-induced atherosclerotic disease through extracellular signal-regulated kinase-1/2 (ERK-1/2) and signal transducer and activator of transcription 3 (STAT 3) phosphorylation. However, there are currently no studies concerning the relationship between AGTR1 polymorphism and hyperhomocysteinemia.
Unfortunately, this study was designed to be cross-sectional with a restricted number of subjects. More studies with a prospective design and a larger number of subjects are needed to confirm our data. Also, only a single gene effect was considered in our study. In many instances, a complex genotype like that for hypertension would require the combined effects of more than two genes.
Naturally, an accurate description of their separate effect is difficult.29) Also, no CC genotype was detected in our study group so the sole effect of the C allele could not be determined. Other factors that can affect blood pressure, such as personal habits and environmental factors were not considered. We included subjects of the same age to exclude a compounding factor that may influence the blood pressure. We could also not determine the duration of hypertension of the study subjects. Not being able to analyze the genotype of the normotensive subjects also remains as one of the limitations of this study.
In conclusion, the AGTR 1 A1166C mutation group had a significantly greater carotid IMT and higher homocysteine levels than the group with the normal genotype of AGTR 1. The AC genotype of AGTR 1 may be useful to predict the presence of early coronary artery disease in hypertensive adolescents. More investigation is necessary to clarify this subject.





 XML Download
XML Download