

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The anomalous origin of the right coronary artery right coronary artery (RCA) is a rare condition,1) but it has clinical importance because there have been reports of nonfatal or fatal myocardial infarction and sudden death associated with exercise for patients with this anatomy.1-3) Because of the high fatality rate associated with this anomaly, most of the published reports that studied large groups of patients have used postmortem diagnoses. The conventional coronary angiogram has limitations with regard to clear visualization of the slitlike ostium of a coronary artery with an anomalous origin. Therefore, intravascular ultrasound (IVUS) for obtaining the cross-sectional luminal image and multidetector row computed tomography (MDCT), which allows threedimensional visualization of the coronary artery with high spatial resolution, may be promising imaging modalities for diagnosing and evaluating this anomaly.4)5) We describe here a patient for whom MDCT was useful to identify this anomaly and IVUS was used for evaluating the myocardial ischemia by visualizing the coronary lumen.
Case
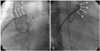
A 22-year-old man presented for evaluation of his effort angina, and he had experienced this for several months. He had no risk factors for coronary artery disease and the resting electrocardiogram (ECG) was normal. He had no history of syncope. Because of the typical angina symptoms, we checked the 64-channel MDCT images for coronary artery disease even though he was young. The 64-channel MDCT scan (Fig. 1) revealed an anomalous origin of the RCA from the left coronary cusp (LCC) with subsequent extrinsic compression between the great vessels (the aorta and main pulmonary artery). After the CT scan, conventional coronary angiography and an IVUS study were performed. According to visual estimation, there was no critical stenotic lesion on the left anterior oblique (LAO) 45°projection view (Fig. 2A); however, a critical stenosis was noted on the right anterior oblique (RAO) 45°projection image (Fig. 2B). The IVUS study showed no atherosclerotic plaque burden on the entire RCA, but a spindle shaped arterial lumen (a slit-like lumen) caused by extrinsic compression was noted from the proximal portion of the RCA to the ostium (Fig. 3A).
Finally, a bypass graft using the right internal mammary artery was performed to prevent myocardial ischemia or sudden cardiac death. The patient has remained asymptomatic after surgery.
Discussion
The causes of myocardial ischemia for this anomaly remain unclear, but the acute angle of the take-off and kinking of the RCA as it arises from the left coronary cusps and also compression of the RCA when it courses within the aortic wall or between the aorta and the pulmonary artery have been thought to be the possible mechanisms.6)7) The myocardial ischemia in this case was presumed to be caused by compression of the anomalous right coronary artery as it coursed between the pulmonary artery and the aorta. Because of the extrinsic compression between the two large vessels, the lumen was squeezed to a spindle shape (a slit-like lumen). This very eccentric lumen narrowing showed relative normal images on the LAO projection views, but a critical stenosis could be seen on the counter RAO projection views in the transverse plane. Therefore, this anomaly can be missed during the conventional angiogram due to this eccentric luminal narrowing.
Several clinical reports on RCA anomalies have beenpreviously reported in Korea,8-10) yet this particular RCA anomaly has not yet been reported on. Invasive coronary angiography was not suitable for our young patient who had no risk factors for a therosclerosis. With the advent of MDCT, noninvasive imaging of coronary artery anatomy has recently become possible. The anomaly of the coronary artery in our case was also easily detected by this noninvasive technique. Future development of MDCT technology should provide higher spatial resolution and this would be more informative for evaluating the mechanisms by which myocardial ischemia is provoked in patients with an anomalous origin of the RCA.


 XML Download
XML Download