

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Echocardiographic evaluation of the left ventricle (LV) long axis function has been reported to be useful for understanding heart failure (HF) with a preserved ejection fraction (EF).1-3) LV peak systolic longitudinal strain (PSLS), as determined using the 2-D speckle tracking method, is a novel indicator of the LV long axis function.4-6) Recently, measurement of the PSLS could be assisted by a newly-developed semi-automated algorithm for automated function imaging (AFI).7) This method can provide quantitative measurements of the global and segmental PSLS and it utilizes a simple bull's eye display.
Diastolic dysfunction (DD), which is regarded as a primary feature of diastolic HF, has been previously evaluated using Doppler studies of mitral inflow and pulmonary venous flow, the left atrial volume indexes (LAVI) and tissue Doppler imaging (TDI) of the mitral annulus.8) Of these parameters, the early diastolic mitral annular (E') velocity and LAVI are commonly regarded as noninvasive indexes of LV relaxation.9)10)
We hypothesized that the patients with a normal EF and DD would have subclinical systolic dysfunction and this could be revealed by measuring the PSLS with using the AFI technique. In the present study, we sought to determine whether the 2-D speckle tracking method could detect subtle change of the LV systolic long axis function via evaluation of the global and segmental PSLS of the LV, and correlation analysis of the PSLS with the conventional parameters that were used to evaluate the diastolic function, such as E' and LAVI.
Subjects and Methods
Study subjects
Comprehensive echocardiographic evaluations were performed in 218 patients. The inclusion criteria used were as follows: 1) stable vital signs, 2) a LV EF >50%, 3) a normal sinus rhythm without left bundle branch block, 4) no regional wall motion abnormality, 5) valvular heart disease (>mild grade) and 6) written informed consent was obtained to participate in the study. After excluding 50 patients who had documented ischemic heart disease with resting wall motion abnormality (n=2), valvular heart disease (n=24), or echocardiographic images unsuitable for analysis (n=24), 168 patients were finally enrolled. This study was approved by the ethical committee of the institutional review board at our hospital.
Echocardiographic examination
Conventional echocardiographic examinations were performed using a Vivid 7® system [General Electrics (GE) Vingmed; Horten Norway] with a 3.5 MHz transducer. Examinations included measurements of the cardiac dimensions, including the interventricular septal thickness (IVST), the LV end-diastolic dimension (EDD), the LV end-systolic dimension (ESD) and the LV posterior wall thickness (PWT) as measured by M-mode echocardiography at the chordae tendineae level. The LV EF was estimated by taking the square of the LV EDD and ESD, as previously described.11) The LAVI values were calculated using the ellipsoidal method.12) The LV mass was calculated by the following formula and it was indexed by the body surface area; LV mass=0.8×(1.04×[LV EDD+IVST+LV PWT]3-[LV EDD]3)+0.6 [gm].11) The relative wall thickness was computed at diastole as follows; (2×LV PWT)/LV EDD.11)
The DD grades were assessed with comprehensive evaluations, i.e., pulsed-wave Doppler examinations of the mitral and pulmonary venous inflow, TDI of the mitral annular velocities (obtained at the septal annulus), and LAVI.12-16) Briefly, the ratio of the mitral inflow early diastolic velocity (E) to the late diastolic velocity (A) was used for the initial DD grading. If the E/A was <0.75, then the patient was categorized into the abnormal relaxation group (grade I DD). If the E/A ratio was in the range of 0.75 to 1.5 and the deceleration time was >140 ms, then the other parameters were used to determine if the diastolic function was normal or pseudonormal (grade II DD).
If there were two or more Doppler indexes suggestive of elevated filling pressures (a change in the E/A with Valsalva of >0.5, a pulmonary venous atrial reversal flow velocity greater than >0.35 m/sec or an E to E' ratio of >10), then the patient was allocated to the grade II DD group. The 168 study subjects were allocated to the grade I DD (n=35), grade II DD (n=45) or normal diastolic function groups (n=59).
Measurement of peak systolic longitudinal strain
The gray scale 2-D harmonic images were obtained in the apical long-axis, 4-chamber and 2-chamber views to determine the PSLS values. All the images were obtained at a frame rate of 60-90 frames/s without dual focus. Three consecutive cardiac cycles were saved in the digital format for off-line analysis and the optimal tracking image was selected for analysis. Strain analysis was performed by one investigator, who was unaware of the patients' DD grades, with using EchoPAC® (BT 06.6.1.0, GE Vingmed) with the AFI technique (Fig. 1). The global PSLS was defined as an average value of the 16 segmental PSLSs of a LV. Additionally, the basal, mid or apical segmental PSLS was defined as an average value of the PSLS of each of the corresponding 6 segments (4 segments for the apex).
Statistical analysis
Statistical analysis was performed using an SAS statistical package (version 9.1, SAS Institute, Cary, NC). The data is presented as means±SDs or as frequencies. One-way analysis of variance with the least significant difference method was used to compare the descriptive parameters after confirming the normal distributions. The 2-tailed Pearson's method was adopted to evaluate the correlations between the PSLS and the other echocardiographic parameters. To investigate the intra- and interpersonal measurement variability, measurements were performed off-line by two investigators on 30 randomly selected cases. The intraclass correlation coefficient of the global PSLS for the intraobserver measurements was 0.90 [n=30, p<0.001, 95% confidence interval (CI) 0.81-0.95], and for interobserver measurements it was 0.91 (n=30, p<0.001, 95% CI 0.81-0.95).
Results
The clinical characteristics and echocardiographic parameters
Of the 168 patients enrolled in this study, the PSLS was measured successfully with good tracking quality in 139 (83%) patients. Their clinical and echocardiographic characteristics according to the DD grade are shown in Table 1. The patients of DD grade I were older than those patients with a normal diastolic function or those patients with grade II DD. Patients with hypertension were more frequently enrolled in the grade II DD group and the systolic blood pressures were higher in this group compared to the other group. The LV EDD and ESD were slightly higher in the grade II DD patients than those values in the grade I DD patients or the normal controls, but there was no significant difference between the LV EF values of these 3 groups. However, the LAVI, the LV mass indexes and the relative wall thickness values were significantly larger in the grade II DD patients as compared to the normal control group. The global and segmental PSLS values in each study group are presented in Table 1. The global and segmental PSLS values were lower in the patients with grade I or II DD than those values in the normal control group. Segmental analysis shows that reductions in the PSLS were more evident in the mid and basal segments (-20.6±1.9% in the normal controls vs. -17.5±2.0% in the DD I patients and -17.5±2.3% in the DD II patients, p<0.001).
Correlations between the segmental PSLS and the echocardiographic parameters
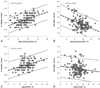
E' was better correlated with the mid and basal PSLS (r=0.510, p<0.001) than with the apical PSLS (r=0.359, p<0.001, Fig. 2). The LAVI also showed a moderate correlation with the mid and basal PSLS (r=-0.422, p<0.001). However, no relationship was found between the LAVI and the apical PSLS (r=-0.137, p=0.109). The LV mass index and the relative wall thickness showed moderate correlation with the mid and basal PSLS (r=0.461, p<0.001 and r=0.507, p<0.001, respectively). However, there was no significant correlation between the relative wall thickness and the apical PSLS (r=0.103, p=0.229), and there was only weak correlation between the LV mass index and the apical PSLS (r=0.191, p=0.024).
Discussion
In this study, we used a newly-developed AFI technique to measure longitudinal 2-D strain. The study demonstrates that the longitudinal systolic functions of the patients with DD, but who had a normal LV EF are lower, in terms of the PSLS, than those of the patients with a normal diastolic function. Furthermore, the global and segmental PSLS are well correlated with the E' velocity and the LAVI, which are commonly used to determine the severity of DD.
HF was previously classified as systolic or diastolic HF with using systolic parameters like the EF and fractional shortening.17) However, there is some debate concerning the diagnosis of diastolic HF and DD. For example, isolated DD can be erroneously diagnosed in a case that displays subtle systolic dysfunction when this is assessed using an imprecise echocardiographic technique, such as the LV EF or fractional shortening by performing M-mode echocardiography. Therefore, a continuum of systolic function was suggested as truly normal function, mildly impaired function that is labeled as diastolic HF, and obviously abnormal LV systolic function.1)18) In these studies, the LV long axis function was measured using LV systolic atrioventricular plane displacement as determined by M-mode echocardiography or the TDI of the mitral annulus.18) The result of our study concerning a decrease in the global PSLS in those patients with DD in the grade I and II groups versus the normal group agree well with those results of the previous studies.
The 2D strain measurements, as determined by speckle tracking, have recently been used for the quantitative evaluation of LV function, and this method has been validated for the evaluation of longitudinal function.5)19) In the current study, we used a semi-automated technique, which has been reported to provide useful rapid measures of the global and segmental PSLS in a routine clinical setting.7) Moreover, the segmental analysis findings can be presented on bull's eye displays by using the AFI technique.
In the present study, the mid and basal segmental PSLS were found to be well correlated with the E', the LV mass index, the relative wall thickness and the LAVI, which are all closely related to the LV diastolic function. These segmental relationships with diastolic function may be due to the fact that the inner myocardium, which is known to be importantly involved in the long axis function, has an oblique fiber orientation.20) This helical orientation might result in the parallel alignment of the longitudinal axis and the inner myocardium only at the mid LV or the base of the LV. On the contrary, the circular fiber orientation of the apical myocardium might result in an intimate relationship between the average clockwise twisting and untwisting rates, which also suggests a close link between systolic contraction and diastolic relaxation.21) DD is a well-known predictor of the clinical outcome in many clinical situations, which include HF with a preserved or reduced EF.22)23) The LV long-axis function, as measured using the systolic amplitude, was recently found to be an independent predictor for survival in HF patients after adjusting for age, gender, heart rate, blood pressure and the EF.24) Considering the good correlations between the diastolic parameters and the quantitative nature of the PSLS, further clinical evaluation of the PSLS with the long-term follow-up is warranted, and especially for the HF patients with a normal EF.
This study has some limitations that should be considered. We could not evaluate the LV diastolic function using invasive parameters such as tau because we considered that cardiac catheterization could not be justified based on the evaluation of diastolic function alone. Secondly, we did not evaluate the strain rate because this could not be obtained using AFI software. However, as strain is a fundamental parameter that can be directly measured using the speckle tracking method, it might be a more relevant parameter than the strain rate, which is in contrast to TDI study. Last, there were no significant differences between the PSLS values in the grade I and II DD patients. Since our grading system for DD did not include an invasive gold standard method, this lack of significant differences might have resulted from the possible errors in the grading process. Therefore, further investigation is required in a future study to determine if PSLS might be useful in grading DD because it could be a sensitive marker for subclinical systolic dysfunction in the patients with DD.
Conclusion
The present study shows that PSLS provides additional information about the diastolic function and subtle systolic dysfunction, and especially concerning the mid and basal LV segments. Therefore, PSLS might be helpful to measure the systolic dysfunction that could be present in the patients who have DD and a normal LV EF.


 XML Download
XML Download