

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Although an anomalous origin of the coronary artery is infrequently encountered, it can cause myocardial ischemia and sudden death in the young, the risk of which mainly depends on the anatomic course taken. In particular, preaortic and; thus, the interarterial pathways of an anomalous left main or right coronary artery, arising from the contralateral sinus and coursing between the aorta and pulmonary trunks, have been reported to be significantly associated with a high risk of sudden cardiac death.1-3) These anomalies are rarely suspected or diagnosed during life, largely due to a lack of clinical suspicion.4) Nevertheless, given the feasibility of surgical correction, timely diagnosis is crucial.
We present a case of a left coronary artery(LCA), with an anomalous origin of the preaortic type, arising from the right sinus of Valsalva and coursing between the aorta and the pulmonary trunks, which culminated in an exercise related myocardial infarction. Transthoracic echocardiographic evaluation, with the Doppler finding of a 'finger-tip phenomenon' allowed the proper diagnosis in this case.
Case
A 14-year-old boy was urgently transferred to our emergency room from a county hospital. He had a history of an episode of syncope, lasting some minutes, during vigorous exercise 2 days previously.
On the day of the event, he suffered parasternal chest pain whilst playing soccer, with subsequent syncope of about 10 minutes duration. On initial examination, his blood pressure was 70/40 mmHg and his heart beat was regular, without definite murmur. Electrocardiography revealed a 2- to 3-mm elevation of the ST segment in V1, V2 and aVL, coupled with a reciprocal change in II, III and aVF(Fig. 1), strongly suggestive of acute myocardial infarction involving the anteroseptal wall. Moreover, this was consistent with the echocardiographic findings, which showed akinesis of the anterior and anteroseptal walls, with a mildly depressed left ventricular ejection fraction of 53%. His cardiac enzyme levels, such as creatine kinase-MB(performed by CX4 PRO, Beckman Coulter) and cardiac troponin-I(performed by VIDAS, bioMerieux), were found to be elevated, at 32.1 ng/mL and 257 IU/L, respectively. Eme rgent coronary angiography was performed, but no significant abnor rgent coronary mality was evident in the right coronary artery. However, adequate cannulation of the LCA to around the usual location failed. Nonselective coronary angiography, by ascending aortography, revealed no evidence of critical stenosis proximal to the mid left anterior descending artery; however, the LCA was suspected to originate from the right sinus of Valsalva. During angiography, his chest pain spontaneously subsided and vital sign stabilized. Meticulous re-evaluation of the transthoracic echocardiography revealed an anomalous origin, at the aortic valve level, of the LCA from the right coronary sinus from the parasternal short axis view. The LCA took a course between the ascending aorta and the pulmonary trunks(Fig. 2A, B). Pulsed wave Doppler echocardiography in the proximal left main coronary artery showed a classic coronary velocity pattern(Fig. 2C); whereas, a 'finger-tip' phenomenon was explicitly exhibited at the distal left main coronary artery, suggesting kinking of the distal left main coronary artery between the ascending aorta and pulmonary trunk(Fig. 2D).
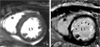
After stabilization, computed tomographic(CT) coronary angiography displayed findings similar to those demonstrated by the transthoracic echocardiography(Fig. 3A, B). 99mTc-MIBI myocardial SPECT showed a severe and reversible perfusion defect in the anterior, anteroseptal and anterolateral walls(Fig. 4) and cardiac magnetic resonance imaging(MRI), with delayed Gd-enhancement, confirmed anterior and anteroseptal myocardial infarction(Fig. 5). Surgical correction of the LCA by reimplantation of the ostium to the left coronary sinus was performed. Intra-operative inspection verified the interarterial course of the LCA. The post-operative recovery was uncomplicated, but he was discharged on the fifth postoperative day.
Discussion
The prevalence of an anomalous origin of the coronary artery has been reported by angiographic series5) and by autopsy series6) to be between 0.2 and 0.3% and 0.3 to 0.5%, respectively. These anomalies are clinically important because they can lead to either acute myocardial infarction or the more severe presentation of sudden cardiac death in the young.
Anomalous LCA from the right sinus of Valsalva is traditionally classified into three different types, according to the anatomic relationship of the aorta and pulmonary trunks.7) Specifically, Type 1 "anomalous" LCA is defined as one crossing the anterior free wall of the right ventricle, Type 2A("interarterial"), courses between the aorta and the pulmonary trunks, Type 2B ("septal"), adopts an intramuscular pathway through the septum, and Type 3, passes to the posterior of the aorta. Of these anomalies, type 2A is remarkable, as it is frequently linked with exertional angina, syncope and sudden cardiac death.8) The incidence of sudden death attributed to type 2A has been reported to be approximately 27%,9) rendering early suspicion and diagnosis imperative for the timely treatment of this inborn coronary abnormality.
However, in the setting of acute myocardial infarction, selective cannulation, through the anomalous origin of the coronary artery, but the detection of its precise course from the 2-D angiography image is often difficult, as in our case.6) Although CT angiography provides the unique facility to undertake 3-D imaging reconstruction of coronary arteries in relation to adjacent anatomical structures, the currently available 16-64 channel CT angiography often requires beta-blocker pretreatment for heart rate control, which is difficult to apply due to the acute decompensating status of left ventricular dysfunction.
In this context, transthoracic echocardiography is a safe and effective tool for the evaluation of a coronary artery with an anomalous origin in the emergent setting or presence of significant left ventricular dysfunction. In addition, transthoracic echocardiographic evaluations of the proximal left and right coronary arteries are feasible and reliable.10) Moreover, Doppler echocardiography can offer information regarding the hemodynamic significance of stenosis. Of note, an early diastolic 'finger-tip' phenomenon, the characteristic Doppler finding of myocardial bridging, can be clearly demonstrated by transthoracic echocardiography.11) This 'finger-tip' coronary flow pattern is characterized by a steep rise in the coronary flow velocity during early diastole, followed by a sharp deceleration and subsequent velocity plateau during mid to late diastole. In our case, the echocardiographic evaluation revealed an anomalous origin of the LCA, with a typical 'finger-tip' coronary flow pattern suggestive of significant hemodynamic disturbance, which aided our correct etiologic diagnosis and decision on surgical correction.
An anomalous origin of a coronary artery is surgically treatable. Coronary bypass graft surgery remains the standard procedure of choice, with excellent long-term results.4) Moreover, thanks to recent advances in surgical techniques, reimplantation of an anomalous coronary artery into the proper coronary sinus can be considered as an alternative.12) Due to our apprehension that the flow of a patent left main coronary artery could compete with a bypass graft, reimplantation of the anomalous coronary artery into the left coronary sinus of Valsalva was concluded to be the more appropriate approach in this case.
We propose that an anomalous origin of a coronary artery must be seriously considered as a potential cause of chest pain or syncope in young patients. A high index of suspicion, with meticulous evaluation by transthoracic echocardiography, can warrant the timely detection of this rare entity.




 XML Download
XML Download