

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background and Objectives
While the clinical significance of descending thoracic aorta intima-media thickness (DTA-IMT) remains unclear, common carotid IMT (CIMT) is known to be associated with major adverse cardiovascular events (MACE) in patients with atherosclerotic disease.
Subjects and Methods
A total of 104 patients (mean age, 59 yrs; 69 male) with angiographically proven coronary atherosclerosis underwent transesophageal echocardiography (TEE) for DTA-IMT measurement and carotid scanning for CIMT measurement. The patients were divided into two groups based on the median IMT value, and they were followed up for cardiovascular events and all-cause mortality for a period of 50±21 months.
Results
Patients having a higher DTA-IMT value (n=44, >2.1 mm) had a higher chance of stroke (6.7% vs. 2.8%, p=0.04), peripheral vascular disease (6.7% vs. 1.9%, p=0.02), and death (2.9% vs. 0%, p=0.04) than those who had lower DTA-IMT values (n=60, ≤2.1 mm). The patients who had higher CIMT values (n=49, >0.089 mm) had a higher chance of peripheral vascular disease (16% vs 2%, p=0.009) than those having lower IMT values (n=55, ≤0.089 mm). However, there was no significant difference between the groups in terms of recurrent chest pain, heart failure, syncope, myocardial infarction or chronic kidney disease during the follow-up period. Multivariate Cox regression analysis revealed that increased DTA-IMT was associated with stroke (OR, 4.29; 95% CI, 1.076-17.181; p=0.039) and peripheral vascular disease (OR, 9.37; 95% CI, 1.571-55.499; p=0.014), whereas increased CIMT was associated with peripheral vascular disease (OR, 14.365; 95% CI, 1.050-196.540; p=0.046).
Figures and Tables
Fig. 1
Descending thoracic aorta IMT was measured in the most thickened wall in the field visualized in end-diastole, except in the area of plaques. The descending aorta was focused upon in the far wall and again a 1 cm long segment was measured at 2mm intervals. The average value of each of the six IMT measurements of the descending thoracic aorta was taken as the evaluable IMT of the aorta. IMT: intima-media thickness.

Fig. 2
Incidence of major adverse cardiovascular event according to the descending thoracic IMT (A) and carotid IMT (B). Base on the descending thoracic aorta IMT mean values, subjects were grouped into high (n=44, ≤0.21 mm) and low IMT (n=60, >0.21 mm). *: statistically significant difference at the 0.05 levels. IMT: intima-media thickness, CHF: congestive heart failure, MI: myocardial infaction, CKD: chronic kidney disease, PVD: peripheral vascular disease.

Fig. 3
Kaplan-Meier curves for event free survival associated with stroke (A), peripheral vascular disease (B), and death (C). Base on the descending thoracic aorta IMT mean values, subjects were grouped into high (n=44, ≤0.21 mm, marked as blanked circle) and low IMT (n=60, >0.21 mm, marked as blanked square). IMT: intima-media thickness.

Fig. 4
Incidence of major adverse cardiovascular event according to the descending thoracic aorta plaque (A) and carotid plaque (B). Base on the presence of descending thoracic aorta plaque, subjects were grouped into present plaque (n=43) and absent plaque (n=61). *: statistically significant difference at the 0.05 levels. CHF: congestive heart failure, MI: myocardial infarction, CKD: chronic kidney disease, PVD: peripheral vascular disease.

Fig. 5
Kaplan-Meier curves for event free survival associated with stroke (A), peripheral vascular disease (B), and death (C). Base on the presence of descending thoracic aorta plaque, subjects were grouped into present plaque (n=43, marked as blanked circle) and absent plaque (n=61, marked as blanked triangle).

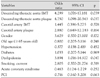
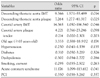
Table 1
Clinical characteristics of the study according to the intima-media thickness of descending thoracic aorta

References
1. Kuller L, Schemanski L, Psaty B, et al. Subclinical disease as an independent risk factor for cardiovascular disease. Circulation. 1995. 92:720–726.
2. O'Leary DH, Polak JF, Wolfson SK Jr, et al. Use of sonography to evaluate carotid atherosclerosis in the elderly. Stroke. 1991. 22:1155–1163.
3. Salonen R, Salonen JT. Determinants of carotid intima-media thickness: a population-based ultrasonography study in eastern Finnish men. J Intern Med. 1991. 229:225–231.
4. Bots ML, Witterman JC, Grobbee DE. Carotid intima-media wall thickness in elderly women with and without atherosclerosis of the abdominal aorta. Atherosclerosis. 1993. 102:99–105.
5. Bae JH, Kim KY. Impact of left ventricular ejection fraction on endothelial function and carotid Intima-media thickness in patients with coronary artery disease. Korean Circ J. 2005. 35:375–381.
6. O'Leary DH, Polak JF, Kronmal RA, Manolio TA, Burke GL, Wolfson SK Jr. Carotid intima-media thickness as a risk factor for myocardial infarction and stroke in older adults. N Engl J Med. 1999. 340:14–22.
7. O'Leary DH, Polak JF, Wolfson SK Jr, et al. Use of sonography to evaluate carotid atherosclerosis in the elderly. Stroke. 1991. 22:1155–1163.
8. Grobbee D, Bots ML. Carotid artery intima-media thickness as a indicator of generalized atherosclerosis. J Intern Med. 1994. 236:567–573.
9. Jeong IB, Bae JH, Kim KY, et al. The carotid intima-media thickness as a screening test for coronary artery disease. Korean Circ J. 2005. 35:460–466.
10. Amarenco P, Cohen A, Tzourio C, et al. Atherosclerotic disease of the aortic arch and the risk of ischemic stroke. N Engl J Med. 1994. 331:1474–1479.
11. Rohani M, Jogestrand T, Ekberg M, et al. Interrelation between the extent of atherosclerosis in the thoracic aorta, carotid intima-media thickness and the extent of coronary artery disease. Atherosclerosis. 2005. 179:311–316.
12. Bae JH, Bassenge E, Park KR, Kim KY, Schwemmer M. Significance of the intima-media thickness of the thoracic aorta in patients with coronary atherosclerosis. Clin Cardiol. 2003. 26:574–578.
13. Lehmann ED, Hopkins KD, Gosling RG. Atherosclerosis in the ascending aorta and risk of ischemic stroke. Lancet. 1995. 346:589–590.
14. Matsumura Y, Takata J, Yabe T, Furuno T, Chikamori T, Doi YL. Atherosclerotic aortic plaque detected by transesophageal echocardiography: its significance and limitation as a marker for coronary artery disease in the elderly. Chest. 1997. 112:81–86.
15. Agarwal R. Estimating GFR from serum creatinine concentration: pitfalls of GFR-estimating equations. Am J Kidney Dis. 2005. 45:610–613.
16. Bostom AG, Kronrnberg F, Ritz E. Predictive performance of renal function equations for patients with chronic kidney disease and normal serum creatinine levels. J Am Soc Nephrol. 2002. 13:2140–2144.
17. Pignoli P, Tremoli E, Poli A, Oreste P, Paoletti R. Intimal plus medial thickness of the arterial wall: a direct measurement with ultrasound imaging. Circulation. 1986. 74:1399–1406.
18. Kallikazaros IE, Tsioufis CP, Stefanadis CI, Pitsavos CE, Toutouzas PK. Closed relation between carotid and ascending aortic atherosclerosis in cardiac patients. Circulation. 2000. 102:III263–III268.
19. Rosvall M, Janzon L, Berglund G, Engstrom G, Hedblad B. Incidence of stroke is related to carotid IMT even in the absence of plaque. Atherosclerosis. 2005. 179:325–331.
20. Fabris F, Zanocchhi M, Fonte G, et al. Carotid plaque, aging, and risk factors: a study of 457 subjects. Stroke. 1994. 25:1133–1140.
21. Spence JD. Ultrsound measurement of carotid plaque as a surrogate outcome for coronary artery disease. Am J Cardiol. 2002. 89:10B–16B.
22. Parfrey PS, Foley RN. The clinical epidemiology of cardiac disease in chronic renal failure. J Am Soc Nephrol. 1999. 10:1606–1615.
23. Fried LF, Shlipak MG, Crump C, et al. Renal insufficiency as a predictor of cardiovascular outcomes and mortality in elderly individuals. J Am Coll Cardiol. 2003. 41:1364–1372.
24. Culleton BF, Larson MG, Wilson PW, Evans JC, Parfrey PS, Levy D. Cardiovascular disease and mortality in a community-based cohort with mild renal insufficiency. Kidney Int. 1999. 56:2214–2219.
 XML Download
XML Download