

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Osteoprotegerin(OPG) is a member of the tumor necrosis factor(TNF) family, and it can function as a soluble decoy receptor by binding with the receptor activator of the nuclear factor-kappa B ligand(RANKL); this competitively inhibits the interaction between RANKL and its receptor.1) OPG is known to inhibit osteoclast proliferation and differentiation, and it has recently been proposed to be linked to osteoporosis and atherosclerosis.2) OPG-deficient mice exhibit severe osteoporosis and multiple artery calcifications in their large arteries.3) Administration of OPG prevented the development of vascular calcification in another animal model of arterial calcifications.4) OPG is also expressed in vitro in vascular cells such as the coronary smooth muscle cells and endothelial cells,5) and it has been shown to prolong endothelial cell survival by preventing apoptosis.6)
OPG is detected not only in normal arteries, but also in the early atherosclerotic lesions of humans.7) These findings suggest that OPG may play a potential role in the process of atherogenesis and atherosclerotic calcification. Recent studies have reported that an increased serum OPG level was significantly associated with the presence and the severity of coronary artery disease,8-10) and also with the cardiovascular mortality of elderly women.11) A recent prospective study reported that elevated OPG levels were an independent risk factor for cardiovascular disease in the general population.12) In addition, it has been suggested that OPG is a novel marker for the cardiovascular mortality and clinical events of patients with acute myocardial infarction(AMI) complicated by heart failure(HF).13) However, no such study has yet been conducted on Asian subjects. Therefore, we measured the serum OPG levels in different patient groups that suffered with HF, unstable angina (UA) and AMI, and we compared the findings with a control group. We also subdivided the study subjects according to the New York Heart Association(NYHA) classification and we then compared the mean serum OPG levels.
Subjects and Methods
Study population
The total study population was 190 subjects(118 males and 72 females, mean age: 60.6±10.5). The study subjects were chosen from the patients who visited the Cardiology Department at Kangbuk Samsung Hospital, Seoul, South Korea from March to November 2005 with the chief complaint of chest pain or dyspnea, after we excluded those patients with non-cardiac diseases and symptoms. The control group consisted of 63 volunteers(32 males and 31 females, mean age: 56.4±8.3), who visited the Kangbuk Samsung Hospital Medical Screening Center for a routine check up on their health status. The study subjects were clinically divided into four groups: the AMI, UA, HF and control groups.
The diagnosis of AMI was determined based on the criteria that satisfied the diagnosis for acute, evolving or recent MI: the typical rise and gradual fall of the troponin levels or a more rapid rise and fall of the CK-MB levels for the biochemical markers of myocardial necrosis, along with at least one of the following: a) ischemic symptoms, b) the development of pathologic Q waves on the ECG, c) ECG changes indicative of ischemia(ST segment elevation or depression) or d) coronary artery intervention(e.g., coronary angioplasty).14) UA was defined as angina pectoris with at least one of three features: 1) it occured at rest and usually lasted more than 20 minutes, 2) it was severe and described as frank pain with a new onset(i.e., within 1 month) and 3) it occurred with a crescendo pattern.15) The diagnosis of HF was made using the Framingham Criteria.16) We regrouped all the subjects according to the NYHA classification and we regarded the control as being in the NYHA I classification.
Those patients with significant concomitant disease such as infection, rheumatoid arthritis, inflammatory bowel disease, chronic renal failure(serum creatinine ≥2.0 mg/dL), chronic liver disease and malignancy, or those patients taking steroids or other immunosuppressants were not included in the study. Informed consent for participation in the study was obtained from all the subjects. The study protocol was reviewed and it was approved by the local ethics committee; the study was performed according to the Declaration of Helsinki.
Measurement of anthropometric data and blood chemistry
The heights, weights, waist circumferences, blood pressures(systolic and diastolic) and heart rates were measured in duplicate and the results were then averaged. The body mass index(BMI) was calculated by dividing the weight(kg) by the height(in meter) squared.
Blood samples were drawn the day after admission. After an overnight fast, the blood glucose, the total cholesterol, triglyceride(TG), high-density lipoprotein cholesterol(HDL-C), low-density lipoprotein cholesterol(LDL-C), blood urea nitrogen(BUN), creatinine, uric acid, the white cell count and the high sensitivity C-reactive protein(hs-CRP) were measured. The hexokinase method was used to measure the blood glucose levels and the enzymatic calorimetric test was used to measure the total cholesterol and triglyceride levels. The selective inhibition method was used to measure the level of HDL-C, and the homogeneous enzymatic calorimetric test was used to measure the level of LDL-C. The serum hs-CRP levels were measured by employing a nephelometric assay and by using a BNII nephelometer(Dade Behring Inc., Deerfield, IL, USA). The results were presented as mg/L and the limit of the measurement was 0.2 mg/L.
Measurement of serum OPG level
To measure the serum OPG, the serum was separated, stored at -80℃ and all the samples were measured simultaneously. The serum OPG levels were measured via sandwich ELISA(Oscotec, Chunan, Korea). In brief, a monoclonal IgG antibody was used as the capture antibody and a biotin-labeled polyclonal anti-human OPG antibody was used as the detection antibody. The intra-assay coefficient of variation was 6.9-9.0%, and the inter-assay coefficient of variation was 6.0-9.0% for the OPG measurement.
Performance of echocardiograms
A two-dimensional echocardiogram was performed for all the subjects to measure the echocardiographic parameters. The internal diameter at end-diastole(IVIDs), the ejection fraction(EF) and the left atrial(LA) size were the parameters we measured.
Statistical analysis
Statistical analysis was performed using SPSS for windows(version 12.0, Chicago, IL). The values were expressed as means and standard deviations(SD). The clinical and biochemical parameters of the study groups were compared by the one-way ANOVA, and post-hoc analysis was performed to individually compare the mean values. The ANCOVA test was used to compare the mean values among the groups after adjustment for age and gender. All multiple comparisons were conducted with the Bonferroni correction. Pearson's correlation analysis was used to determine the correlation between the OPG levels for each of the variables we studied. Multiple regression analysis with using the serum OPG level at the time of diagnosis was performed to determine the predictors after adjustment for confounding factors. All the subjects were regrouped according to the NYHA classification, and another multiple regression analysis was then performed. p<0.05 were considered as significantly different.
Results
Baseline characteristics
The study subjects consisted of 190 subjects; these included 118 males and 72 females(mean age: 60.6±10.5) (Table 1). We divided the patients into four groups according to their disease status, and we also divided them by the NYHA classifications(Table 2). There were 28 patients in the HF group, 53 patients in the UA group, 46 patients in the AMI group and 63 subjects in the control group.
Comparison of the serum OPG levels among the groups, as divided by the disease status and the NYHA classification
There was a significant difference in the mean age across the groups; the patients in the HF, UA and AMI groups were older than those in the control group(p<0.001). The mean age and ejection fraction(EF) for the control, UA, AMI and HF groups were 56±8, 62±10, 61±13 and 68±9, and 67±7%, 66±8%, 52±15% and 42±13%, respectively(p<0.001 and p<0.001).
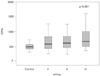
The mean values of the serum OPG levels were more elevated in the HF, UA and AMI groups than in the control group, and these differences were significant even after adjustment for age and gender(p<0.001)(Fig. 1).
Relationship between the serum OPG level and the cardiovascular risk factors, the disease status and the NYHA classification
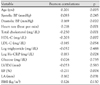
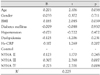
Correlation analyses were performed between the serum OPG level and the various cardiovascular risk factors in the control group(Table 3). Positive correlations were observed between the serum OPG levels and the patients' age, heart rates and log HsCRP; negative correlations were observed for total cholesterol, HDL-C and the EF. When multiple regression analysis was performed with the serum OPG level as the dependent variable and the cardiovascular risk factors and disease status as the independent variables, the presence of HF and AMI were significant positive predictors of the serum OPG levels after adjustment was made for the confounding variables, including the EF(p=0.030, p=0.001, respectively).
When multiple regression analysis was performed with the serum OPG level as the dependent variable and the NYHA classification as the independent variable, positive correlations were detected between the serum OPG levels and the NYHA III and IV classifications after adjustment for the confounding factors(Table 4, p=0.007, p=0.008).
Discussion
The present study showed that patients suffering with AMI and HF had significantly increased serum OPG levels compared with the controls. In addition, the serum OPG levels were significantly more elevated in the NYHA III and IV groups than that in the NYHA I group.
A recent report demonstrated that the serum OPG level was significantly elevated in the patients suffering with AMI complicated by HF13); another study reported that the systemic expression of RANKL and OPG increased according to the functional, hemodynamic and neurohormonal disease severity in human HF.14) Our findings are consistent with the above reports and it is one of a few studies suggesting an association between the serum OPG levels and heart failure, and it is the first one performed on non-Caucasians.
We cannot define the precise mechanism associated with increased serum OPG levels in patients suffering with AMI and HF since OPG is known to be a product of many tissues, including the organs of the cardiovascular system, the lungs, kidneys, bone and the circulating immune cells.17) Moreover, we cannot derive any conclusions regarding the relative contributions of ischemia and HF, respectively, to the increased OPG levels in patients suffering with AMI and HF. Although recent studies have reported high levels of OPG in patients with angina,8)9) another study found increased OPG levels in chronic HF patients with no differences observed between the patients suffering with ischemic or idiopathic cardiomyopathy.19) This result suggests that HF in itself is a potent stimulus for the release of OPG.
The enhanced systemic expression of RANKL was accompanied by the expression of RANKL/RANK by the cardiomyocytes in both human and rat models of HF.17) These findings suggest a potential role for RANKL/RANK interaction in the pathogenesis of HF that involves endocrine, paracrine and autocrine mechanisms such as the interactions between infiltrating activated T cells and cardiomyocytes. OPG can prevent interaction between RANK and RANKL by binding to RANKL. Thus, an increased serum OPG level in patients with HF could potentially protect against the deleterious effects of RANKL. Although the stabilizing effect of OPG on RANKL cannot be excluded, the pathophysiological consequences of the increased serum OPG level in HF patients must be further studied. Furthermore, if the serum RANKL level could be measured simultaneously with the OPG level, then questions about the effects of OPG on RANKL would be solved easier. In this study we showed that the OPG level was elevated in AMI subjects after adjusting for EF. We can speculate that OPG plays a protective role by its expression in vascular smooth muscle cells and in the endothelium in response to pro-apoptotic stimuli, since vascular apoptosis can weaken the cap tissue and thereby promote plaque rupture.6)19) In addition, recent studies have also shown that serum OPG is more highly secreted in symptomatic carotid plaques than in the asymptomatic lesions.20) Therefore, it could be hypothesized that the increased serum OPG levels in AMI patients may result from the rupture of plaques. Another explanation of OPG's role may be via the collagen network. Disruption of this collagen network may lead to myocyte slippage, ventricular dilatation and progressive contractile dysfunction.21-23) The M matrix-degrading enzyme family probably plays a role in determining the integrity of the tissue in an atherosclerotic plaque, as well as during the process of plaque rupture.20-23) Therefore, OPG may play a major role in the ventricular remodeling and dilatation seen in HF patients; OPG influences the plaque vulnerability by modulating these enzymes directly or by OPG's binding to RANKL.
Our finding of higher serum OPG levels in AMI patients may be related to the increased secretion of inflammatory cytokine that occur in patients with acute coronary syndromes.24-26) In vitro studies have shown that inflammatory cytokines such as PDGF, IL-1 and TNF-alpha upregulate the OPG expression in vascular smooth muscle and endothelial cells.27) Thus, we measured the Hs-CRP, which is an acute-phase reactant, as a novel marker of atherosclerosis. We found simple correlation between the serum OPG level and the Hs-CRP level. This finding is consistent with other studies that have shown a relationship between the OPG level and the systemic inflammatory markers.10)11)
This study has several limitations. First, there were significant differences in age, gender and the number of subjects among the different study groups. Further, we did not analyze the menopausal status, which might have influenced the serum OPG level. However, there were consistent significant differences in the serum OPG levels among the groups even after adjustment for age and gender. Therefore, this limitation was unlikely to have affected the results. However, further investigations are needed that will employ well-characterized, well-matched study groups. Second, the control group was a volunteer sample population and not a random sample of the general community. Third, the blood samples were drawn the day after admission, so the OPG level might have been influenced by the acute phase, but we did not measure the follow-up OPG levels and we did not measure the BNP, which is a surrogate marker of heart disease. Further study is needed to learn whether the OPG and BNP levels decline in patients with severe heart failure after they undergo adequate treatment. Finally, the number of subjects was relatively small. Thus, we expect that any extended future studies will include a larger, random population sample.
In conclusion, we have shown that the serum OPG levels were increased in patients with cardiovascular disease such as HF and AMI, and also with the NYHA classification in Asian subjects. The serum OPG level could be a novel marker for different stages of cardiovascular disease.


 XML Download
XML Download