

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Coronary air embolism is an uncommon complication during coronary angiography and angioplasty, and the incidence of this depends on the operator's experience and awareness. The complications of air embolism range from a clinically insignificant event to an acute coronary syndrome and death. Treatment has consisted of supportive measures, the use of 100% oxygen and pain relief. The use of various mechanical interventions have also been reported.1-3)
We describe here a rare case of massive air embolism to the left coronary arteries during elective percutaneous coronary intervention(PCI), and this caused cardiogenic shock.
Case
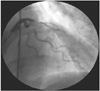
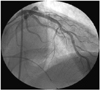
A 52-year-old man was admitted for coronary angiography because of anterior chest pain that occurred at dawn 10 days previously. His risk factor was smoking. Coronary angiogram showed a critical stenosis in the middle left anterior descending artery(LAD)(Fig. 1), and PCI was planned for the LAD lesion. After passage of the guide-wire over the lesion site, blood pressure tracing curves were abnormally demonstrated on the pressure screen monitor. We manipulated the saline infusion-pressure gauge tubing system and manifold to correct the unusual demonstration. After verifying the blood pressure, the blood pressure tracing curves were normal. A balloon catheter was then advanced over the lesion site. Immediately after an initial injection of to check the proper location of the balloon, the patient began to complain of severe chest pain and profound perspiration. Wide QRS ventricular complexes(40 beats/min) and ST-segment elevations were demonstrated on the ECG monitor and his blood pressure was decreased to 50/30 mmHg. An emergency coronary angiogram showed air columns in the proximal LAD and left circumflex artery(LCX), which interrupted the total coronary flow(Fig. 2). With the diagnosis of air embolism, cardiac massage was immediately performed with giving 100% oxygen through a facial mask and intravenous administration of 0.5 mg atropine. Hydration, intravenous dopamine 10 ug/kg/min and temporary pacing were also started. In spite of those treatments, the patient still remained hemodynamically unstable and the air columns were not washed out on repeated fluoroscopic examinations(Fig. 3). Thus, we injected contrast media and 200 µg nitroglycerin twice successively. About 7 to 8 minutes after the acute event, he gradually recovered from the shock state and his chest pain disappeared. After the air embolism had disappeared, the patient successfully underwent stent implantation at the lesion site(Fig. 4). There was no elevation of cardiac enzymes after the PCI and he was discharged uneventfully one week later.
Discussion
Although it is rare and preventable, coronary air embolism is still a part of the inevitable complications of coronary angiography and angioplasty. The estimated incidence of significant coronary air embolism might approach 0.19% in the hands of a new trainee, and the total incidence is 0.27% when including the unnoticed or unreported asymptomatic air embolisms.1)
The possible mechanisms of introducing air into the coronary artery include incomplete aspiration of the angiographic or guiding catheters, balloon rupture, insinuation of air with balloon catheter introduction or withdrawal, structural failures of the equipment and the constant negative suction of self-venting catheters that are left outside the body.1)4) In our patient, inadvertent manipulation of the pressure gauge tubing system and manifold seemed to have permitted entrance of air.
Coronary air embolim should be differentiated from clot injection, spasm and coronary dissection. The typical appearance of air in the coronary artery during contrast injection is at the leading edge of the contrast media, and it terminates abruptly with a hazy appearance that pulsates back and forth on a meniscus of air.5) A clot can be outlined by contrast material, and the leading edge of the contrast media does not pulsate back and forth.6) In addition, a clot usually produces a single occlusion at a bifurcation. Coronary artery dissection occurs near the tip of the catheter and this often produces a characteristic appearance with a flap, a narrowed segment and local persistence of contrast media in the false lumen.7)
The consequences of coronary air embolism depend on the amount of air introduced into the coronary vessels. A study on dogs showed that intracoronary injection of 0.02 mL/kg of air caused death in 28% of the animals.8) In another study on pigs, injection of micro air bubbles at a volume of 2 µL/kg to the LAD artery resulted in a significant reduction of segmental contractility.9) The myocardial injury was determined by the sizes of these micro air bubbles.
Adequate management of this complication has not been established because these cases usually remain unreported due to the clinicians' reluctance to discuss the complications of their work.
The vast majority of observed emboli are extremely small volumes of air that do not result in symptoms or hemodynamic consequences; therefore, they require no therapy. For the mild to moderately symptomatic episodes, routine management consists of 100% oxygen by face mask, analgesics for chest pain, monitoring and treating arrhythmia and supporting the patients as necessary for the few minutes it takes for the air to clear spontaneously. In the event that massive air embolism occurs, like our case, aggressive efforts to reestablish the coronary blood flow as soon as possible are essential to reduce injury to the myocardium and to speed recovery from the hemodynamic crisis. High-dose inotropic agents and intraaortic balloon counterpulsation have been used in that regard.10)
Some debate can exist for our case as to whether severe microvascular spasm occurred. Yet vasospasm is common in the setting of air embolization and the vasospastic mechanism at the proximal coronary segment plays a deleterious effect on the microvasculature by causing a decrease in the capillary bed space that leads to a decrease in the distal coronary blood flow,11) and this can ultimately mimic the situation of microvascular spasm.
It is not certain whether our patient recovered spontaneously with supportive measures as time went by or he recovered dramatically by the direct action of intracoronary nitroglycerin. It has been proved that nitroglycerin causes dilatation of the epicardial coronary artery and microcirculation. Thus, a more dilated coronary vessel could have a higher coronary driving force and much more surface contact between the inhaled 100% oxygen and the air emboli. These effects facilitate the passage and absorption of the air bubbles. So, we carefully suggest that intracoronary nitroglycerin can be the additional treatment for the coronary air embolism that is non-responsive general supportive care.


 XML Download
XML Download