

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
In the recent 10 to 15 years, the most popular issue in the spine field is evaluation and treatment of the sagittal alignment and sagittal balance of the spine. Adult spine deformity (ASD) includes not only coronal deformity, such as degenerative scoliosis, but also sagittal deformity. Degenerative scoliosis is also associated with sagittal deformity of the spine. Even in degenerative scoliosis, accompanying sagittal deformity is more important to clinical symptoms than coronal deformity. Sagittal deformity of the spine is significantly correlated with health-related quality of life score, such as visual analogue scale and Oswestry disability index, short form-36 health survey. For the appropriate evaluation and treatment of ASD, understanding the normal and abnormal sagittal alignment and sagittal balance of the spine is very important. Various compensatory mechanisms should be applied in order to maintain the balanced upright posture. Assessment of the compensatory mechanism is also mandatory for proper surgical planning. Some spinopelvic parameters show particularly high correlation with clinical symptoms in case of sagittal imbalance. Therefore, assessment of these parameters is necessary for evaluation of surgical outcomes.
Figures and Tables
 | Figure 1SRS-Schwab classification system. An individual's coronal curve pattern is categorized, and, most importantly, each of 3 sagittal modifiers (PI-LL, SVA, and PT) is classified as 'nonpathological (0),' 'moderate deformity (+),' or 'marked deformity (++).' SRS, Scoliosis Research Society; PI, pelvic incidence; LL, lumbar lordosis; SVA, sagittal vertical axis; PT, pelvic tilt.
|
 | Figure 2Segmental angles. Lower most two segments, L4 and L5 comprised of approximately 70% of maximum lumbar lordosis. Restoration of these two segmental angles is very important for restoration of adequate sagittal balance.
|
 | Figure 3Jackson's pelvic radius technique for measurement of pelvic morphology and pelvic balance around both hips. HASP, the distance between hip axis and sacral promontory; HAS1, the distance between hip axis and posterior superior corner of S1; pelvic radius (PR), distance between the center of the hip axis and the S1 reference point; pelvic angle (PA), angle of rotational pelvic balance around the hip joint; PR-S1, pelvic morphology which does not change regardless of pelvic rotation; Ant., anterior; Post., posterior; SS, sacral slope; PI, pelvic incidence.
|
 | Figure 4Pelvic parameters. Positional parameters; pelvic tilt, sacral slope and overhang, morphologic parameters; pelvic incidence and pelvic thickness.
|
 | Figure 5Demonstration of relationship between pelvic incidence and pelvic tilt in compensatory adjustment for kyphosis. Smaller pelvic incidence indicates less compensatory ability. PI, pelvic incidence; SS, sacral slope; PT, pelvic tilt.
|
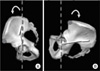
 | Figure 6(A) Model and lateral X-ray of a low-grade pelvic incidence pelvis (vertical pelvis). Note the high position of the L5 S1 disc with respect to the top of the iliac crest. (B) High grade pelvic incidence pelvis (horizontal pelvis). L5 S1 disc and L5 are totally below the top of the iliac crest.
|
 | Figure 7(A) Left maximum pelvis anterior rotation: which is the same as a complete hip flexion and can facilitate hip dislocation. (B) Right maximum pelvis posterior rotation: which shows the limit of pelvis backtilt (the extension reserve).
|
 | Figure 8Parameters of the sagittal balance of the spine and pelvis. The spinal balance is defined as the horizontal offset between the midsacral point and C7 plumb line; spinopelvic balance, between hip axis and C7 plumb line; and sacropelvic balance, between hip axis and midsacral point.
|
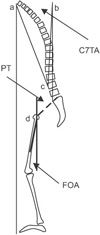 | Figure 9Preoperative planning using the full balance integrated technique. C7 translation angle: C7TA. Midpoint of the C7 inferior plateau (a) is translated on the plumb line ascending from the mid part of the S1 plateau (b). Point c is on the anterior cortex of the selected vertebra for osteotomy, which is mainly L4 vertebra. Femur obliquity angle: FOA. Femur flexion is measured as the angle between the femoral axis and the plumb line (d). Pelvis compensation angle: PTA. Pelvic tilt is measured as usual: line between center femoral head to mid part of S1 plateau and vertical line. If PT between 15° and 25°: add 5°. If PT superior 25°: add 10°. PT, pelvic tilt.
|
 | Figure 10Measurement of global spinal balance. (A) Spinosacral angle; (B) spinal tilt; and (C) C7 translation ratio.
|
 | Figure 11Spinopelvic angle (SPA) formed by the line between the center of the C7 body and the center of the S1 upper endplate and the line between the center of the S1 upper endplate and hip axis. SPA combines the spinosacral angle (SSA) and pelvisacral angle, the pelvic morphologic angle. Therefore, SPA consider not only positional parameter but also anatomical parameter.
|
 | Figure 12T1 pelvic angle (TPA), a novel radiographic parameter that accounts for both global malalignment and compensation through pelvic retroversion. The TPA is defined as the angle between the line from the femoral head axis to the centroid of T1 and the line from the femoral head axis to the middle of the S1 superior end plate. The TPA is the sum of the T1 spinopelvic inclination (T1SPi) and the pelvic tilt (PT).
|
 | Figure 13Incliniation of spine over the hip joint. T1 Spinopelvic inclination and T9 spinopelvic inclination defined as the angle between the vertical plumbline and the line drawn from the vertebral body center of T1 or T9 and the center of the bicoxofemoral axis.
|
 | Figure 14Mechanism for acquisition of upright posture. Two main mechanisms, first, hip extension with verticalization of the sacrum by contraction of the gluteal muscle and hamstring muscle and relaxation of the anterior tension band to make hip extension easier and second, making lordosis with horizontalization of the sacrum by the erector spinae muscle and tightening of the anterior tension band to prevent or limit hip overextension. This mechanism is also applied as a compensatory mechanism for maintaining sagittal balance.
|
 | Figure 15New pelvic parameters; femoropelvic angle (FPA) and femoral tilt angle (FTA) (asterisks). Note that pelvic tilt (PT) is equal to the sum of FPA and FTA. Cited from the article of Lee et al. (Eur Spine J. 2013;22:1059-65).84)
|
 | Figure 16Two different responses according to the knee flexion. (A) Standing without knee and hip flexion. The angle of femoropelvic angle (FPA) (asterisks) is equal to pelvic tilt (PT). (B) No pelvic compensation. Note that FPA does not change and PT increases with knee flexion. (C) Pelvic compensation. Note that PT does not change and FPA decreases with knee flexion Cited from the article of Lee et al. (Eur Spine J. 2013;22:1059-65).84) FTA, femoral tilt angle.
|
 | Figure 17Realignment objectives in the sagittal plane. Sagittal vertical axis (SVA)<50 mm, pelvic tilt (PT)<20°, and lumbar lordosis (LL)=pelvic incidence (PI)±9° sets the stage for achievement of a successful harmonious spinopelvic realignment.
|
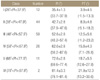
Table 1
Classes of PI and Corresponding Values of Spinopelvic Positional Parameters from a Control Group of 154 Subjects
![]()


References
1. Schwab F, Dubey A, Gamez L, et al. Adult scoliosis: prevalence, SF-36, and nutritional parameters in an elderly volunteer population. Spine (Phila Pa 1976). 2005; 30:1082–1085.

2. Glassman SD, Bridwell K, Dimar JR, Horton W, Berven S, Schwab F. The impact of positive sagittal balance in adult spinal deformity. Spine (Phila Pa 1976). 2005; 30:2024–2029.
3. Lafage V, Schwab F, Patel A, Hawkinson N, Farcy JP. Pelvic tilt and truncal inclination: two key radiographic parameters in the setting of adults with spinal deformity. Spine (Phila Pa 1976). 2009; 34:E599–E606.
4. Schwab FJ, Patel A, Shaffrey CI, et al. Sagittal realignment failures following pedicle subtraction osteotomy surgery: are we doing enough?: Clinical article. J Neurosurg Spine. 2012; 16:539–546.
5. Schwab F, Patel A, Ungar B, Farcy JP, Lafage V. Adult spinal deformity-postoperative standing imbalance: how much can you tolerate? An overview of key parameters in assessing alignment and planning corrective surgery. Spine (Phila Pa 1976). 2010; 35:2224–2231.
6. Schwab F, el-Fegoun AB, Gamez L, Goodman H, Farcy JP. A lumbar classification of scoliosis in the adult patient: preliminary approach. Spine (Phila Pa 1976). 2005; 30:1670–1673.
7. Schwab F, Farcy JP, Bridwell K, et al. A clinical impact classification of scoliosis in the adult. Spine (Phila Pa 1976). 2006; 31:2109–2114.
8. Schwab F, Lafage V, Farcy JP, et al. Surgical rates and operative outcome analysis in thoracolumbar and lumbar major adult scoliosis: application of the new adult deformity classification. Spine (Phila Pa 1976). 2007; 32:2723–2730.
9. Duval-Beaupère G, Robain G. Visualization on full spine radiographs of the anatomical connections of the centres of the segmental body mass supported by each vertebra and measured in vivo. Int Orthop. 1987; 11:261–269.
10. Lafage V, Schwab F, Skalli W, et al. Standing balance and sagittal plane spinal deformity: analysis of spinopelvic and gravity line parameters. Spine (Phila Pa 1976). 2008; 33:1572–1578.
11. Legaye J, Duval-Beaupère G. Sagittal plane alignment of the spine and gravity: a radiological and clinical evaluation. Acta Orthop Belg. 2005; 71:213–220.
12. Legaye J, Duval-Beaupère G, Hecquet J, Marty C. Pelvic incidence: a fundamental pelvic parameter for three-dimensional regulation of spinal sagittal curves. Eur Spine J. 1998; 7:99–103.
13. Schwab FJ, Blondel B, Bess S, et al. International Spine Study Group (ISSG). Radiographical spinopelvic parameters and disability in the setting of adult spinal deformity: a prospective multicenter analysis. Spine (Phila Pa 1976). 2013; 38:E803–E812.
14. Schwab F, Ungar B, Blondel B, et al. Scoliosis Research Society-Schwab adult spinal deformity classification: a validation study. Spine (Phila Pa 1976). 2012; 37:1077–1082.
15. Schwab F, Lafage V, Patel A, Farcy JP. Sagittal plane considerations and the pelvis in the adult patient. Spine (Phila Pa 1976). 2009; 34:1828–1833.
16. Schwab F, Bess S, Blondel B, et al. Combined assessment of pelvic tilt, pelvic incidence/lumbar lordosis mismatch and sagittal vertical axis predicts disability in adult spinal deformity: a prospective analysis. Spine. Supplement 2011 SRS Society Meeting Abstract. Louisville (KY): Spine;2011.
17. Schwab F, Lafage V, Shaffrey C, et al. Pre-operative pelvic parameters must be considered to achieve adequate sagittal balance after lumbar osteotomy. Paper presented at: International Meeting for Advanced Spinal Techniques. 2009 Jul 15-18; Vienna, Austria.
18. Jackson RP. The sagittal plane-from birth to the grave: spinopelvic alignment and balance. In : CME course, SRS meeting; 1997.
19. Peterson MD, Nelson LM, McManus AC, Jackson RP. The effect of operative position on lumbar lordosis. A radiographic study of patients under anesthesia in the prone and 90-90 positions. Spine (Phila Pa 1976). 1995; 20:1419–1424.
20. Stagnara P, De Mauroy JC, Dran G, et al. Reciprocal angulation of vertebral bodies in a sagittal plane: approach to references for the evaluation of kyphosis and lordosis. Spine (Phila Pa 1976). 1982; 7:335–342.
21. Roussouly P, Pinheiro-Franco JL. Sagittal parameters of the spine: biomechanical approach. Eur Spine J. 2011; 20:Suppl 5. 578–585.
22. Bernhardt M, Bridwell KH. Segmental analysis of the sagittal plane alignment of the normal thoracic and lumbar spines and thoracolumbar junction. Spine (Phila Pa 1976). 1989; 14:717–721.
23. Gelb DE, Lenke LG, Bridwell KH, Blanke K, McEnery KW. An analysis of sagittal spinal alignment in 100 asymptomatic middle and older aged volunteers. Spine (Phila Pa 1976). 1995; 20:1351–1358.
24. Jackson RP, McManus AC. Radiographic analysis of sagittal plane alignment and balance in standing volunteers and patients with low back pain matched for age, sex, and size. A prospective controlled clinical study. Spine (Phila Pa 1976). 1994; 19:1611–1618.
25. Bradford DS. Juvenile kyphosis. In : Lonstein JE, Winter RB, Bradford DS, Ogilvie JW, editors. Moe's textbook of scoliosis and other spinal deformities. 3rd ed. Philadelphia: Saunders;1994. p. 349–367.
26. Lee CS, Oh WH, Chung SS, Lee SG, Lee JY. Analysis of the sagittal alignment of normal spines. J Korean Orthop Assoc. 1999; 34:949–954.
27. Voutsinas SA, MacEwen GD. Sagittal profiles of the spine. Clin Orthop Relat Res. 1986; 210:235–242.
28. Hardacker JW, Shuford RF, Capicotto PN, Pryor PW. Radiographic standing cervical segmental alignment in adult volunteers without neck symptoms. Spine (Phila Pa 1976). 1997; 22:1472–1480.
29. Boulay C, Tardieu C, Hecquet J, et al. Sagittal alignment of spine and pelvis regulated by pelvic incidence: standard values and prediction of lordosis. Eur Spine J. 2006; 15:415–422.
30. Debarge R, Demey G, Roussouly P. Sagittal balance analysis after pedicle subtraction osteotomy in ankylosing spondylitis. Eur Spine J. 2011; 20:Suppl 5. 619–625.
31. Kim YJ, Bridwell KH, Lenke LG, Rhim S, Cheh G. An analysis of sagittal spinal alignment following long adult lumbar instrumentation and fusion to L5 or S1: can we predict ideal lumbar lordosis? Spine (Phila Pa 1976). 2006; 31:2343–2352.
32. Blondel B, Schwab F, Bess S, et al. Posterior global malalignment after osteotomy for sagittal plane deformity: it happens and here is why. Spine (Phila Pa 1976). 2013; 38:E394–E401.
33. Marnay T. Equilibre du rachis et du bassin. Cahiers d'enseignement de la SOFCOT. 1988. p. 281–331.
34. During J, Goudfrooij H, Keessen W, Beeker TW, Crowe A. Toward standards for posture. Postural characteristics of the lower back system in normal and pathologic conditions. Spine (Phila Pa 1976). 1985; 10:83–87.
35. Duval-Beaupère G, Schmidt C, Cosson P. A barycentremetric study of the sagittal shape of spine and pelvis: the conditions required for an economic standing position. Ann Biomed Eng. 1992; 20:451–462.
36. Jackson RP, Kanemura T, Kawakami N, Hales C. Lumbopelvic lordosis and pelvic balance on repeated standing lateral radiographs of adult volunteers and untreated patients with constant low back pain. Spine (Phila Pa 1976). 2000; 25:575–586.
37. Jackson RP, Peterson MD, McManus AC, Hales C. Compensatory spinopelvic balance over the hip axis and better reliability in measuring lordosis to the pelvic radius on standing lateral radiographs of adult volunteers and patients. Spine (Phila Pa 1976). 1998; 23:1750–1767.
38. Vialle R, Levassor N, Rillardon L, Templier A, Skalli W, Guigui P. Radiographic analysis of the sagittal alignment and balance of the spine in asymptomatic subjects. J Bone Joint Surg Am. 2005; 87:260–267.
39. Lazennec JY, Riwan A, Gravez F, et al. Hip spine relationships: application to total hip arthroplasty. Hip Int. 2007; 17:Suppl 5. S91–S104.
40. Vaz G, Roussouly P, Berthonnaud E, Dimnet J. Sagittal morphology and equilibrium of pelvis and spine. Eur Spine J. 2002; 11:80–87.
41. Mac-Thiong JM, Roussouly P, Berthonnaud E, Guigui P. Sagittal parameters of global spinal balance: normative values from a prospective cohort of seven hundred nine Caucasian asymptomatic adults. Spine (Phila Pa 1976). 2010; 35:E1193–E1198.
42. Le Huec JC, Aunoble S, Philippe L, Nicolas P. Pelvic parameters: origin and significance. Eur Spine J. 2011; 20:Suppl 5. 564–571.
43. Mac-Thiong JM, Berthonnaud E, Dimar JR 2nd, Betz RR, Labelle H. Sagittal alignment of the spine and pelvis during growth. Spine (Phila Pa 1976). 2004; 29:1642–1647.
44. Berthonnaud E, Dimnet J, Roussouly P, Labelle H. Analysis of the sagittal balance of the spine and pelvis using shape and orientation parameters. J Spinal Disord Tech. 2005; 18:40–47.
45. Boulay C, Tardieu C, Hecquet J, et al. Anatomical reliability of two fundamental radiological and clinical pelvic parameters: incidence and thickness. Eur J Orthop Surg Traumatol. 2005; 15:197–204.
46. Barrey C. Equilibre sagittal pelvi-rachidien et pathologies lombaires dégénératives. Etude comparative à propos de 100 cas [in French] [thesis]. Lyon: Claude Bernard University Lyon 1;2004.
47. Barrey C, Jund J, Noseda O, Roussouly P. Sagittal balance of the pelvis-spine complex and lumbar degenerative diseases. A comparative study about 85 cases. Eur Spine J. 2007; 16:1459–1467.
48. Jang JS, Lee SH, Min JH, Maeng DH. Changes in sagittal alignment after restoration of lower lumbar lordosis in patients with degenerative flat back syndrome. J Neurosurg Spine. 2007; 7:387–392.
49. Roussouly P, Berthonnaud E, Dimnet J. Geometrical and mechanical analysis of lumbar lordosis in an asymptomatic population: proposed classification. Rev Chir Orthop Reparatrice Appar Mot. 2003; 89:632–639.
50. Roussouly P, Nnadi C. Sagittal plane deformity: an overview of interpretation and management. Eur Spine J. 2010; 19:1824–1836.
51. Mangione P, Sénégas J. Sagittal balance of the spine. Rev Chir Orthop Reparatrice Appar Mot. 1997; 83:22–32.
52. Descamps H, Commare-Nordamn MC, Marty C, et al. Modification of pelvic angle during the human growth. Biom Hum Anthrpol. 1999; 17:59–63.
53. Labelle H, Roussouly P, Berthonnaud E, et al. Spondylolisthesis, pelvic incidence, and spinopelvic balance: a correlation study. Spine (Phila Pa 1976). 2004; 29:2049–2054.
54. Mangione P, Gomez D, Senegas J. Study of the course of the incidence angle during growth. Eur Spine J. 1997; 6:163–167.
55. Mac-Thiong JM, Roussouly P, Berthonnaud E, Guigui P. Ageand sex-related variations in sagittal sacropelvic morphology and balance in asymptomatic adults. Eur Spine J. 2011; 20:Suppl 5. 572–577.
56. Lazennec JY, Ramaré S, Arafati N, et al. Sagittal alignment in lumbosacral fusion: relations between radiological parameters and pain. Eur Spine J. 2000; 9:47–55.
57. Mendoza-Lattes S, Ries Z, Gao Y, Weinstein SL. Natural history of spinopelvic alignment differs from symptomatic deformity of the spine. Spine (Phila Pa 1976). 2010; 35:E792–E798.
58. Vrtovec T, Janssen MM, Likar B, Castelein RM, Viergever MA, Pernuš F. Evaluation of pelvic morphology in the sagittal plane. Spine J. 2013; 13:1500–1509.
59. Vrtovec T, Janssen MM, Likar B, Castelein RM, Viergever MA, Pernuš F. A review of methods for evaluating the quantitative parameters of sagittal pelvic alignment. Spine J. 2012; 12:433–446.
60. Lee CS, Chung SS, Kang KC, Park SJ, Shin SK. Normal patterns of sagittal alignment of the spine in young adults radiological analysis in a Korean population. Spine (Phila Pa 1976). 2011; 36:E1648–E1654.
61. Roussouly P, Pinheiro-Franco JL. Biomechanical analysis of the spino-pelvic organization and adaptation in pathology. Eur Spine J. 2011; 20:Suppl 5. 609–618.
62. Lee CS, Chung SS, Chung KH, Kim SR. Significance of pelvic incidence in the development of abnormal sagittal alignment. J Korean Orthop Assoc. 2006; 41:274–280.
63. Vidal J, Marnay T. Morphology and anteroposterior body equilibrium in spondylolisthesis L5-S1. Rev Chir Orthop Reparatrice Appar Mot. 1983; 69:17–28.
64. Vidal J, Marnay T. Sagittal deviations of the spine, and trial of classification as a function of the pelvic balance. Rev Chir Orthop Reparatrice Appar Mot. 1984; 70:Suppl 2. 124–126.
65. Dubousset J. Three-dimensional analysis of the scoliotic deformity. In : Weinstein SL, editor. The pediatric spine: principles and practice. New York: Raven Press;1994.
66. Mac-Thiong JM, Transfeldt EE, Mehbod AA, et al. Can c7 plumbline and gravity line predict health related quality of life in adult scoliosis? Spine (Phila Pa 1976). 2009; 34:E519–E527.
67. Glassman SD, Berven S, Bridwell K, Horton W, Dimar JR. Correlation of radiographic parameters and clinical symptoms in adult scoliosis. Spine (Phila Pa 1976). 2005; 30:682–688.
68. Booth KC, Bridwell KH, Lenke LG, Baldus CR, Blanke KM. Complications and predictive factors for the successful treatment of flatback deformity (fixed sagittal imbalance). Spine (Phila Pa 1976). 1999; 24:1712–1720.
69. Lafage V, Bharucha NJ, Schwab F, et al. Multicenter validation of a formula predicting postoperative spinopelvic alignment. J Neurosurg Spine. 2012; 16:15–21.
70. Rose PS, Bridwell KH, Lenke LG, et al. Role of pelvic incidence, thoracic kyphosis, and patient factors on sagittal plane correction following pedicle subtraction osteotomy. Spine (Phila Pa 1976). 2009; 34:785–791.
71. Klineberg E, Schwab F, Smith JS, Gupta MC, Lafage V, Bess S. Sagittal spinal pelvic alignment. Neurosurg Clin N Am. 2013; 24:157–162.
72. Le Huec JC, Leijssen P, Duarte M, Aunoble S. Thoracolumbar imbalance analysis for osteotomy planification using a new method: FBI technique. Eur Spine J. 2011; 20:Suppl 5. 669–680.
73. Roussouly P, Gollogly S, Noseda O, Berthonnaud E, Dimnet J. The vertical projection of the sum of the ground reactive forces of a standing patient is not the same as the C7 plumb line: a radiographic study of the sagittal alignment of 153 asymptomatic volunteers. Spine (Phila Pa 1976). 2006; 31:E320–E325.
74. Protopsaltis T, Schwab F, Bronsard N, et al. TheT1 pelvic angle, a novel radiographic measure of global sagittal deformity, accounts for both spinal inclination and pelvic tilt and correlates with health-related quality of life. J Bone Joint Surg Am. 2014; 96:1631–1640.
75. Ryan DJ, Protopsaltis TS, Ames CP, et al. T1 pelvic angle (TPA) effectively evaluates sagittal deformity and assesses radiographical surgical outcomes longitudinally. Spine (Phila Pa 1976). 2014; 39:1203–1210.
76. Legaye J, Hecquet J, Marty C, Duval-Beaupere G. Equilibre sagittal du rachis. Relations entre bassin et courbures rachidiennes sagittales en position debout. Rachis. 1993; 5:215–226.
77. Duval-Beaupère G, Legaye J. Composante sagittale de la statique rachidienne. Rev Rhum. 2004; 71:105–119.
78. Barrey C, Roussouly P, Perrin G, Le Huec JC. Sagittal balance disorders in severe degenerative spine. Can we identify the compensatory mechanisms. Eur Spine J. 2011; 20:Suppl 5. 626–633.
79. Abitbol MM. Evolution of the lumbosacral angle. Am J Phys Anthropol. 1987; 72:361–372.
80. Paquet N, Malouin F, Richards CL. Hip-spine movement interaction and muscle activation patterns during sagittal trunk movements in low back pain patients. Spine (Phila Pa 1976). 1994; 19:596–603.
81. Nakada K. A study on senile postural deformity. Nihon Seikeigeka Gakkai Zasshi. 1988; 62:1149–1161.
82. Lee CS, Lee CK, Kim YT, Hong YM, Yoo JH. Dynamic sagittal imbalance of the spine in degenerative flat back: significance of pelvic tilt in surgical treatment. Spine (Phila Pa 1976). 2001; 26:2029–2035.
83. Westhuizen JVD. Spinal balance in scoliosis. Geneva: Big Time Spine;2000.
84. Lee CS, Park SJ, Chung SS, Lee KH. The effect of simulated knee flexion on sagittal spinal alignment: novel interpretation of spinopelvic alignment. Eur Spine J. 2013; 22:1059–1065.
85. Vosse D, van der Heijde D, Landewé R, et al. Determinants of hyperkyphosis in patients with ankylosing spondylitis. Ann Rheum Dis. 2006; 65:770–774.
86. Schwab FJ, Smith VA, Biserni M, Gamez L, Farcy JP, Pagala M. Adult scoliosis: a quantitative radiographic and clinical analysis. Spine (Phila Pa 1976). 2002; 27:387–392.
87. Djurasovic M, Glassman SD. Correlation of radiographic and clinical findings in spinal deformities. Neurosurg Clin N Am. 2007; 18:223–227.
88. Ames CP, Smith JS, Scheer JK, et al. Impact of spinopelvic alignment on decision making in deformity surgery in adults: A review. J Neurosurg Spine. 2012; 16:547–564.
89. Skalli W, Zeller RD, Miladi L, et al. Importance of pelvic compensation in posture and motion after posterior spinal fusion using CD instrumentation for idiopathic scoliosis. Spine (Phila Pa 1976). 2006; 31:E359–E366.
 XML Download
XML Download