

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
The purpose of this study was to analyze patient factors including smoking, body mass index, correction angle, graft material, presence of lateral cortex fracture, and age for the effect on bone union after open-wedge high tibial osteotomy and the effect of graft material used for lateral cortex fractures.
Materials and Methods
This retrospective study was conducted on 54 patients and 58 cases with osteoarthritic change Kallgren-Lawrence grade 2 or less from May 2012 to June 2014. Average follow-up period was 22 months (14–38 months). The patients were divided into two groups according to patient related factors and graft materials (allograft, n=6; beta-tricalcium phosphate [β-TCP], n=6) used for lateral cortex fractures and were analyzed for the relationship with bone union after open-wedge high tibial osteotomy. Radiographic and clinic analyses were performed, and van Hemert grading was used for grading bone union at 6 weeks, 3 months, 6 months, and 1 year postoperatively.
Results
The non-smoking group and the group without lateral cortex fracture showed significantly higher bone union rates than the control group. No significant clinical or radiological difference was observed between the two groups in 12 cases and the allograft group showed significantly higher rates of union at 6 months and 1 year postoperatively according to the van Hemert grading.
Figures and Tables



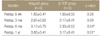
Table 4
Demographic Data of Patients in the Allograft Group and β-TCP Group with Lateral Cortex Fracture
![]()


References
1. Ministry for Health and Welfare. Elderly real state survey. Seoul: Ministry for Health and Welfare;2009.
2. Jackson JP, Waugh W. Tibial osteotomy for osteoarthritis of the knee. J Bone Joint Surg Br. 1961; 43-B:746–751.

3. Coventry MB. Osteotomy about the knee for degenerative and rheumatoid arthritis. J Bone Joint Surg Am. 1973; 55:23–48.
4. Benzakour T, Hefti A, Lemseffer M, El Ahmadi JD, Bouyarmane H, Benzakour A. High tibial osteotomy for medial osteoarthritis of the knee: 15 years follow-up. Int Orthop. 2010; 34:209–215.
5. Keene JS, Dyreby JR Jr. High tibial osteotomy in the treatment of osteoarthritis of the knee. The role of preoperative arthroscopy. J Bone Joint Surg Am. 1983; 65:36–42.
6. Staeheli JW, Cass JR, Morrey BF. Condylar total knee arthroplasty after failed proximal tibial osteotomy. J Bone Joint Surg Am. 1987; 69:28–31.
7. Brouwer RW, Bierma-Zeinstra SM, van Raaij TM, Verhaar JA. Osteotomy for medial compartment arthritis of the knee using a closing wedge or an opening wedge controlled by a Puddu plate. A one-year randomised, controlled study. J Bone Joint Surg Br. 2006; 88:1454–1459.
8. Spahn G. Complications in high tibial (medial opening wedge) osteotomy. Arch Orthop Trauma Surg. 2004; 124:649–653.
9. van den Bekerom MP, Patt TW, Kleinhout MY, van der Vis HM, Albers GH. Early complications after high tibial osteotomy: a comparison of two techniques. J Knee Surg. 2008; 21:68–74.
10. Agneskirchner JD, Freiling D, Hurschler C, Lobenhoffer P. Primary stability of four different implants for opening wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2006; 14:291–300.
11. Stoffel K, Stachowiak G, Kuster M. Open wedge high tibial osteotomy: biomechanical investigation of the modified Arthrex Osteotomy Plate (Puddu Plate) and the TomoFix Plate. Clin Biomech (Bristol, Avon). 2004; 19:944–950.
12. van Raaij TM, Brouwer RW, de Vlieger R, Reijman M, Verhaar JA. Opposite cortical fracture in high tibial osteotomy: lateral closing compared to the medial opening-wedge technique. Acta Orthop. 2008; 79:508–514.
13. Brown CW, Orme TJ, Richardson HD. The rate of pseudarthrosis (surgical nonunion) in patients who are smokers and patients who are nonsmokers: a comparison study. Spine (Phila Pa 1976). 1986; 11:942–943.
14. Meidinger G, Imhoff AB, Paul J, Kirchhoff C, Sauerschnig M, Hinterwimmer S. May smokers and overweight patients be treated with a medial open-wedge HTO? Risk factors for non-union. Knee Surg Sports Traumatol Arthrosc. 2011; 19:333–339.
15. Sloan A, Hussain I, Maqsood M, Eremin O, El-Sheemy M. The effects of smoking on fracture healing. Surgeon. 2010; 8:111–116.
16. Lobenhoffer P, Agneskirchner J, Zoch W. Open valgus alignment osteotomy of the proximal tibia with fixation by medial plate fixator (in German). Orthopade. 2004; 33:153–160.
17. Staubli AE, De Simoni C, Babst R, Lobenhoffer P. TomoFix: a new LCP-concept for open wedge osteotomy of the medial proximal tibia: early results in 92 cases. Injury. 2003; 34:Suppl 2. B55–B62.
18. van Hemert WL, Willems K, Anderson PG, van Heerwaarden RJ, Wymenga AB. Tricalcium phosphate granules or rigid wedge preforms in open wedge high tibial osteotomy: a radiological study with a new evaluation system. Knee. 2004; 11:451–456.
19. Jensen JA, Goodson WH, Hopf HW, Hunt TK. Cigarette smoking decreases tissue oxygen. Arch Surg. 1991; 126:1131–1134.
20. Sarin CL, Austin JC, Nickel WO. Effects of smoking on digital blood-flow velocity. JAMA. 1974; 229:1327–1328.
21. Jones JK, Triplett RG. The relationship of cigarette smoking to impaired intraoral wound healing: a review of evidence and implications for patient care. J Oral Maxillofac Surg. 1992; 50:237–239. discussion 239-40.
22. Harvey EJ, Agel J, Selznick HS, Champman JR, Henley MB. Deleterious effect of smoking on healing of open tibia-shaft fractures. Am J Orthop (Belle Mead NJ). 2002; 31:518–521.
23. Miller BS, Dorsey WO, Bryant CR, Austin JC. The effect of lateral cortex disruption and repair in the stability of the medial opening wedge high tibial osteotomy. Am J Sports Med. 2005; 33:1552–1557.
24. Yacobucci GN, Cocking MR. Union of medial opening-wedge high tibial osteotomy using a corticocancellous proximal tibial wedge allograft. Am J Sports Med. 2008; 36:713–719.
25. Esenkaya I, Elmali N. Proximal tibia medial open-wedge osteotomy using plates with wedges: early results in 58 cases. Knee Surg Sports Traumatol Arthrosc. 2006; 14:955–961.
26. Santic V, Tudor A, Sestan B, Legovic D, Sirola L, Rakovac I. Bone allograft provides bone healing in the medial opening high tibial osteotomy. Int Orthop. 2010; 34:225–229.
27. Cho SW, Kim DH, Lee GC, Lee SH, Park SH. Comparison between autogenous bone graft and allogenous cancellous bone graft in medial open wedge high tibial osteotomy with 2-year follow-up. Knee Surg Relat Res. 2013; 25:117–125.
28. Gouin F, Yaouanc F, Waast D, Melchior B, Delecrin J, Passuti N. Open wedge high tibial osteotomies: calcium-phosphate ceramic spacer versus autologous bonegraft. Orthop Traumatol Surg Res. 2010; 96:637–645.
 XML Download
XML Download