

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Gout often occurs in the first metatarsophalyngeal joint, and also in the ankle joint and posterior foot. Knee joint gouty arthritis is commonly reported, but gouty tophi in bilateral popliteal cysts, such as this case, are rare. We report on a case treated by cystectomy of gouty tophi in bilateral popliteal cysts and review.
Figures and Tables
Figure 1
(A) Gross finding on both popliteal areas. Approximately 70×60 mm sized firm and round masses are palpated on both popliteal areas. (B) Gross finding on the right 5th finger. Approximately 40×30 mm sized firm and whitish mass on the right 5th proximal interphalangeal joint.

Figure 2
(A) Preoperative lateral radiograph of the right knee. (B) Preoperative lateral radiograph of the left knee. Soft tissue masses are seen.
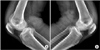
Figure 3
(A) Magnetic resonance imaging (MRI) of the right knee with T2-weighted fat suppression sagittal view shows diffuse calcified synovial thickening in the knee joint, with large calcified mass formation (approximately 6 cm in the long axis) in popliteal fossa. (B) MRI of the left knee T2-weighted. Sagittal view shows diffuse calcified synovial thickening in the knee joint, with large calcified mass formation (approximately 7.5 cm in the long axis) in popliteal fossa.
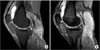
Figure 4
Tc-99m hydroxydiphosphonate (HDP) whole body bone scan showed a soft tissue mass with faint increased uptake behind both knee joints. Increased uptake is shown on both knee joints, left ankle joint, right elbow joint and other multiple joints.


References
1. Weselman KO, Agudelo CA. Gout basics. Bull Rheum Dis. 2001; 50:1–3.
2. Chung TG, Kim HG, Song YS, et al. Clinical manifestations of gout in Korea. Korean J Med. 1997; 53:84–92.
3. Agudelo CA, Wise CM. Gout: diagnosis, pathogenesis, and clinical manifestations. Curr Opin Rheumatol. 2001; 13:234–239.

4. Bickel WH, Burleson RJ, Dahlin DC. Popliteal cyst; a clinicopathological survey. J Bone Joint Surg Am. 1956; 38:1265–1274.
5. Nakano KK. Entrapment neuropathy from Baker's cyst. JAMA. 1978; 239:135.
6. Scott WN, Jacobs B, Lockshin MD. Posterior compartment syndrome resulting from a dissecting popliteal cyst. Case report. Clin Orthop Relat Res. 1977; 122:189–192.
7. Hong KD, Ha SS, Shim JC. Tophaceous gout involving the bipartitle patella: a case report. J Korean Knee Soc. 2000; 12:226–229.
8. Lim HC, Shim JH, Nam HW, Choi BS, Hong MP. Pathologic quadriceps tendon rupture in patients with chronic renal failure: case report. J Korean Knee Soc. 2000; 12:234–238.
9. Jeong JC, Park CH, Cho HK, et al. Gouty tophus on the tibial tuberosity with accompanied chemical cellulitis localized at the upper tibia. J Korean Rheum Assoc. 2004; 11:183–187.
10. Park RY, Nam SY, Lee JH, et al. A case of ruptured popliteal cyst in gouty arthritis. J Korean Rheum Assoc. 2002; 9:308–312.
 XML Download
XML Download