

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Figures and Tables
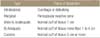
 | Figure 1Surgical margin. Cited from the article of Enneking (Instr Course Lect. 1988;37:3-10)10) with original copyright holder's permission.
|
 | Figure 2Surgical margin from Kawaguchi. The principle of curative wide resection is that, when a barrier exists, the tumor is removed outside the barrier. When a barrier is not present, the tumor is removed using as much margin as possible greater than 5 cm. (A) In case of a skin or subcutaneous lesion, the lesion is removed with a margin of 5 cm or more where the barrier does not exist and outside the barrier where it does exist. (B) If the lesion arises in an intermuscular area, the margin is more than 5 cm where there is no barrier. (C) In intramuscular lesions, the muscle surrounding the tumor is removed 5 cm from the reactive zone where a barrier does not exist, and the dissection and resection of the nearby tissues depends on the barrier rather than the true physical distance from the lesion. (D) In bone sarcoma, the tumor is removed 5 cm from the lesion if a barrier does not exist like the site of the nearby diaphysis of the bone but if a barrier exists the barriers are converted into equivalent distances and the tumor is removed accordingly. Cited from the article by Kawaguchi et al. (Clin Orthop Relat Res. 2004;419:165-72)9) with original copyright holder's permission.
|
 | Figure 3Case 1. (A) A 27-year-old female who underwent planned excision. (A) Preoperative plain radiograph. (B) Coronal, saggital, axial view of the magnetic resonance imaging taken before a planned surgical treatment. (C) Gross clinical photograph of the widely excised tumor. (D) Postoperative plain radiograph.
|
 | Figure 4Case 2. A 15-year-old female who undedrwent planned excision. (A) Preoperative plain radiograph. (B) Coronal, saggital, axial view of the magnetic resonance imaging taken before a planned surgical treatment. (C) Gross clinical photograph of the widely excised tumor. (D) Postoperative plain radiograph.
|
Table 1
Definition of TNM and Grade

Cited from Edge et al. (Springer-Verlag, 2009)7) with original copyright holder's permission. *Because of the rarity of lymph node involvement in sarcomas, the designation NX may not be appropriate and could be considered N0 if no clinical involvement is evident. †Ewing's sarcoma is classified as G4.
![]()
Table 2
Staging Grouping of AJCC

Cited from Edge et al. (Springer-Verlag, 2009)7) with original copyright holder's permission. AJCC, American Joint Committee on Cancer.
![]()
Table 3
Musculoskeletal Tumor Society Staging System

Cited from the article of Enneking et al. (Clin Orthop Relat Res. 1980; 153:106-20)8) with original copyright holder's permission.
![]()
Table 4
Surgical Grading of Bone and Soft Tissue Sarcomas

Cited from the article of Kawaguchi et al. (Clin Orthop Relat Res. 2004;419:165-72)9) with original copyright holder's permission.
![]()
Table 5
Musculoskeletal Oncologic Surgery from Enneking

Cited from the article of Enneking (Instr Course Lect. 1988;37:3-10)10) with original copyright holder's permission.
![]()
Table 6
Surgical Margins for Bone and Soft Tissue Sarcomas
Cited from the article of Kawaguchi et al. (Clin Orthop Relat Res. 2004;419:165-72)9) with original copyright holder's permission.
![]()
Table 7
Evaluation of the Response of the Tumor to Preoperative Chemotherapy or Radiotherapy or Both

Cited from the article of Kawaguchi et al. (Clin Orthop Relat Res. 2004;419:165-72)9) with original copyright holder's permission. MR, marked response; PR, partial response; NC, no change of local disease; PD, progressive local disease.
![]()
Table 8
Relationship between Local Curability and Surgical Procedures

Cited from the article of Kawaguchi et al. (Clin Orthop Relat Res. 2004;419:165-72)9) with original copyright holder's permission.
![]()
 XML Download
XML Download