

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Soft tissue tumors are classified into benign and malignant on the basis of the patient's age, medical history, physical examination, pathological and radiologic examination. We have to caution against misdiagnosis of malignant tumor which can delay the treatment time. Lipoma, schwannoma, hemangioma, and ganglion cysts are common benign tumors, usually of small size and are often located in the superficial layer. Although it may be suspected as a benign tumor, performing contrast-enhanced magnetic resonance maging is preferably advantageous. Liposarcoma and undifferentiated pleomorphic sarcoma, the most common malignant soft tissue tumors, usually occur after middle age; rhabdomyosarcoma is usually presented in children and synovial sarcoma often occurs at a younger age. The magnetic resonance (MR) signal intensity of lipoma shows uniformity with subcutaneous fat, sarcoma should be suspected if it has a contrast-enhanced and non-fat-suppressed part. The MR signals of ganglion cysts show homogeneous and same signal intensity with joint fluid and urine, while the liquid containing sarcoma, like synovial sarcoma, is characterized by heterogeneous signal intensity and contrast enhancement. If surgery is performed, an incision should be made in the longitudinal direction of the limb and the excised tumor should be sent for pathology analysis. When the macroscopic finding of the tumor during surgery is different from the expected diagnosis, the operation should cease with biopsy only or the small superficial tumor can be excised widely if possible. The transfer should be considered unless you can be sure of a benign tumor in hands and feet of children. When diagnosed as malignant tumors, patients should be provided with sufficient information that can lead them to a musculoskeletal tumor specialist.
Figures and Tables

Figure 2
Synovial sarcoma can be confused with the popliteal cyst. T2 sagittal (A) and axial magnetic resonance images (B) show heterogeneous signal intensity with fluid-fluid level. (C) Synovial sarcoma has a contrast enhancement portion.

Figure 3
Lipogenic tumor should be compared with the subcutaneous fat layer of the magnetic resonance imaging signal. (A) Lipoma has totally the same signal as the subcutaneous fat layer in T1 (left), fat suppression (middle) and contrast enhancement (right). (B) A well-differentiated liposarcoma with deep location (left), nonfat suppression area (middle; arrow) and thick septum with enhancement area (right; arrow).
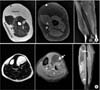
Figure 4
Undifferentiated pleomorphic sarcoma. Sarcoma is suspected, if the superficially located tumor shows a different signal than the subcutaneous fat layer (A) and has contrast enhancement (B).

Figure 5
Wide excisional biopsy. (A) A superficially located tumor of the arm shows a different signal compared with the subcutaneous fat layer. (B, C) The cephalic vein is compressed. (D) Superficial nerves and blood vessels in contact with sarcoma should be excised without dissection. (E) An excised sarcoma should be covered with normal tissues in all directions.

Figure 6
Benign soft tissue tumors in the hand show different magnetic resonance signals schwannoma (A), lipoma (B), and hemangioma (C).

Figure 7
Synovial sarcoma of the finger shows more contrast enhancement (A) than a giant cell tumor of the tendon sheath (B).

Figure 8
Remember, the colors of soft tissue tumors. Lioma (A), schwannoma (B), and hemangioma (C) is distinguished by the color of sarcoma (D).

Figure 9
(A) If intraoperatively, superficial tumor tissue differs from expected benign, wide excision can be performed before or after biopsy result. (B) The color of the sarcoma is quite different from that of subcutaneous fat tissue.


Table 1
AJCC Staging for Soft Tissue Sarcomas

Cited from the article of Edge et al. (Springer, 2010).14)
Table 2
Surgical Staging System by the Musculoskeletal Tumor Society

Cited from the aricle of Enneking et al. (Clin Orthop Relat Res. 1980;153:106-20).11)


Notes
References
1. Fletcher CD. The evolving classification of soft tissue tumours: an update based on the new WHO classification. Histopathology. 2006; 48:3–12.

2. Fletcher CDM, Unni KK, Mertens FE. Pathology and genetics of tumours of soft tissue and bone. World Health Organization classification of tumours. Lyon: IARC Press;2002.
3. Coindre JM. New WHO classification of tumours of soft tissue and bone. Ann Pathol. 2012; 32:S115–S116.
4. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2006. CA Cancer J Clin. 2006; 56:106–130.
5. Peabody TD, Gibbs CP Jr, Simon MA. Evaluation and staging of musculoskeletal neoplasms. J Bone Joint Surg Am. 1998; 80:1204–1218.
6. Peabody TD, Simon MA. Principles of staging of soft-tissue sarcomas. Clin Orthop Relat Res. 1993; 289:19–31.
7. Russell WO, Cohen J, Enzinger F, et al. A clinical and pathological staging system for soft tissue sarcomas. Cancer. 1977; 40:1562–1570.
8. Beahrs OH, Henson DE, Hutter RVP, et al. Manual for staging of cancer. 4th ed. Philadelphia: Lippincott;1992.
9. Fleming ID, Cooper JS, Henson GE, et al. AJCC cancer staging manual. 5th ed. Philadelphia: Lippincott-Raven;1997.
10. Enneking WF. Musculoskeletal tumor surgery. New York: Churchill Livingstone;1983.
11. Enneking WF, Spanier SS, Goodman MA. A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop Relat Res. 1980; 153:106–120.
12. Enneking WF, Spanier SS, Malawer MM. The effect of the anatomic setting on the results of surgical procedures for soft parts sarcoma of the thigh. Cancer. 1981; 47:1005–1022.
13. Greene FL, Page DL, Fleming ID, et al. AJCC cancer staging manual. 6th ed. New York: Springer-Verlag;2002.
14. Edge SB, Byrd DR, Compton CC, et al. AJCC cancer staging manual. 7th ed. New York: Springer;2010.
15. Urakawa H, Tsukushi S, Arai E, et al. Association of short duration from initial symptoms to specialist consultation with poor survival in soft-tissue sarcomas. Am J Clin Oncol. 2015; 38:266–271.
16. Stramare R, Beltrame V, Gazzola M, et al. Imaging of soft-tissue tumors. J Magn Reson Imaging. 2013; 37:791–804.
17. Aga P, Singh R, Parihar A, Parashari U. Imaging spectrum in soft tissue sarcomas. Indian J Surg Oncol. 2011; 2:271–279.
18. Littrup PJ, Bang HJ, Currier BP, et al. Soft-tissue cryoablation in diffuse locations: feasibility and intermediate term outcomes. J Vasc Interv Radiol. 2013; 24:1817–1825.
19. Umer HM, Umer M, Qadir I, Abbasi N, Masood N. Impact of unplanned excision on prognosis of patients with extremity soft tissue sarcoma. Sarcoma. 2013; 2013:498604.
20. Kang S, Han I, Lee SA, Cho HS, Kim HS. Unplanned excision of soft tissue sarcoma: the impact of the referring hospital. Surg Oncol. 2013; 22:e17–e22.
21. Nishimura A, Matsumine A, Asanuma K, et al. The adverse effect of an unplanned surgical excision of foot soft tissue sarcoma. World J Surg Oncol. 2011; 9:160.
22. Qureshi YA, Huddy JR, Miller JD, Strauss DC, Thomas JM, Hayes AJ. Unplanned excision of soft tissue sarcoma results in increased rates of local recurrence despite full further oncological treatment. Ann Surg Oncol. 2012; 19:871–877.
23. Han I, Kang HG, Kang SC, Choi JR, Kim HS. Does delayed reexcision affect outcome after unplanned excision for soft tissue sarcoma? Clin Orthop Relat Res. 2011; 469:877–883.
 XML Download
XML Download