

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Interventional pain management by percutaneous epidural neuroplasty (PEN) has potential as a useful treatment method in chronic low back and/or radicular pain that is refractory to other conservative treatments. The effect of PEN is known to result from targeting of drug delivery to areas of pathology in the spinal epidural space. The procedure involves removing barriers, such as epidural fibrosis, that prevent drug from reaching target sites. Therefore, the goal during lysis of epidural adhesions is to penetrate mechanical barriers impeding injected material from spreading effectively into the areas of pathology in the epidural space by the catheter. An additional lavage effect, reducing the local concentration of proinflammatory substances seems possible. Although a true mechanical lysis of postsurgical adhesions or scar tissues by means of PEN appears to be impossible because it has been proven by experimental biomechanical study, mild to moderate adhesions may be broken up by a PEN catheter allowing the medications to reach the target site through the new channel made by the catheter. This review will focus on the adhesiolysis technique using the sacral hiatus approach in treatment of chronic low back pain with/without lumbosacral radiculopathy.
Figures and Tables
Figure 1
(A) Skin incision was made 1cm lateral and 2cm inferior to the sacral hiatus (arrow). (B) Insert guide needle into sacral hiatus via skin incision. P, proximal; D, distal (gluteal fold).
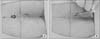
Figure 2
(A) Magnetic resonance imaging shows that the beginning point of the dural sac (arrow) is at the 2nd sacral body. (B) Do not insert guide needle above the 3rd sacral body to avoid inadvertent dural puncture.

Figure 3
Place some degree of bend (arrow) in the catheter tip to make advancement to the ventrolateral side of the desired lesion site much easier.

Figure 4
After confirming ventrolateral catheter placement of the catheter in anteroposterior (AP) and lateral views under fluoroscopic visualization, inject 1.5 ml of contrast media to visualize and document dye spread into area of pathology and outline the targeted nerve root. Rule out vascular, subdural or subarachnoid injection during this process. (A) AP view. (B) Lateral view.

Figure 5
(A) If the patient has multiple levels of pathology, divide dosage of drugs according to the levels and at first, catheter tip (arrow) is placed in the most proximal level (L3, 4 in this figure) and inject divided dosage. (B) Then withdraw the catheter tip (arrow) from the proximal level to the distal level (L4, 5 in this figure) for injection.

Figure 6
Pain control manipulator (PCM) has a steerable catheter with a handle and an atraumatic tip. From above, wire (inserts into lumen of catheter), PCM catheter, needle spacer (fills guide needle), guide needle.

Figure 7
Magnetic resonance imaging shows the fragment (arrows) of the catheter which was inserted and broken at another hospital. (A) T2-weighted sagittal image. (B) Gadolinium enhanced sagittal image. (C) T2-weighted coronal image.

Figure 8
(A) If the catheter is bent at the bevel side of the needle (arrow), shearing of the catheter can be made during movement of the catheter. (B) Rotate bevel needle to prevent catheter from shearing.

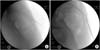
Figure 9
(A) In the epidural space, contrast media spreads asymmetrically with multiple small sized filling defects. The margin of dye spread is irregular. (B) After dural puncture, contrast media spreads symmetrically without filling defects. This is the myelogram that has a smooth margin of dye.

Figure 10
(A) It is impossible to insert a device into the epidural space in case of obliteration or severe stenosis in sacral hiatus or canal. In that case, authors developed a method that hand drilling can provide the entry for needle and catheter. (B) Using a guide needle as an introducer, K-wire with hand drill is an alternative method to secure the pathway.
References
1. Manchikanti L, Helm Ii S, Pampati V, Racz GB. Percutaneous adhesiolysis procedures in the medicare population: analysis of utilization and growth patterns from 2000 to 2011. Pain Physician. 2014; 17:E129–E139.
2. Chan CW, Peng P. Failed back surgery syndrome. Pain Med. 2011; 12:577–606.

3. Hsu E, Atanelov L, Plunkett AR, Chai N, Chen Y, Cohen SP. Epidural lysis of adhesions for failed back surgery and spinal stenosis: factors associated with treatment outcome. Anesth Analg. 2014; 118:215–224.
4. Veihelmann A, Devens C, Trouillier H, Birkenmaier C, Gerdesmeyer L, Refior HJ. Epidural neuroplasty versus physiotherapy to relieve pain in patients with sciatica: a prospective randomized blinded clinical trial. J Orthop Sci. 2006; 11:365–369.
5. Veihelmann A. The significance of immunology in orthopaedics today. Orthopade. 2003; 32:736–743.
6. Specchia N, Pagnotta A, Toesca A, Greco F. Cytokines and growth factors in the protruded intervertebral disc of the lumbar spine. Eur Spine J. 2002; 11:145–151.
7. Ozaktay AC, Cavanaugh JM, Asik I, DeLeo JA, Weinstein JN. Dorsal root sensitivity to interleukin-1 beta, interleukin-6 and tumor necrosis factor in rats. Eur Spine J. 2002; 11:467–475.
8. Heavner JE, Racz GB, Raj P. Percutaneous epidural neuroplasty: prospective evaluation of 0.9% NaCl versus 10% NaCl with or without hyaluronidase. Reg Anesth Pain Med. 1999; 24:202–207.
9. Abdi S, Datta S, Trescot AM, et al. Epidural steroids in the management of chronic spinal pain: a systematic review. Pain Physician. 2007; 10:185–212.
10. Devulder J, Bogaert L, Castille F, Moerman A, Rolly G. Relevance of epidurography and epidural adhesiolysis in chronic failed back surgery patients. Clin J Pain. 1995; 11:147–150.
11. Lee JH, Lee SH. Clinical effectiveness of percutaneous adhesiolysis using Navicath for the management of chronic pain due to lumbosacral disc herniation. Pain Physician. 2012; 15:213–221.
12. Birkenmaier C, Baumert S, Schroeder C, Jansson V, Wegener B. A biomechanical evaluation of the epidural neurolysis procedure. Pain Physician. 2012; 15:E89–E97.
13. Manchikanti L, Bakhit CE. Percutaneous lysis of epidural adhesions. Pain Physician. 2000; 3:46–64.
14. Kim JH, Jung HJ, Nahm FS, Lee PB. Does improvement in epidurography following percutaneous epidural neuroplasty correspond to patient outcome? Pain pract. Published online April 21, 2014. DOI: 10.1111/papr.12197.
15. Rydell N, Balazs EA. Effect of intra-articular injection of hyaluronic acid on the clinical symptoms of osteoarthritis and on granulation tissue formation. Clin Orthop Relat Res. 1971; 80:25–32.
16. Helm S. A review of the role of epidural percutaneous adhesiolysis. Pain Manag. 2012; 2:609–616.
17. Helm Ii S, Benyamin RM, Chopra P, Deer TR, Justiz R. Percutaneous adhesiolysis in the management of chronic low back pain in post lumbar surgery syndrome and spinal stenosis: a systematic review. Pain Physician. 2012; 15:E435–E462.
18. Kim SB, Kim MK, Kim KD, Lim YJ. Unintended complication of intracranial subdural hematoma after percutaneous epidural neuroplasty. J Korean Neurosurg Soc. 2014; 55:170–172.
19. Sekiguchi M, Yabuki S, Satoh K, Kikuchi S. An anatomic study of the sacral hiatus: a basis for successful caudal epidural block. Clin J Pain. 2004; 20:51–54.
20. Jo DH, Yang HJ, Kim JJ. Approach for epiduroscopic laser neural decompression in case of the sacral canal stenosis. Korean J Pain. 2013; 26:392–395.
21. Gerdesmeyer L, Wagenpfeil S, Birkenmaier C, et al. Percutaneous epidural lysis of adhesions in chronic lumbar radicular pain: a randomized, double-blind, placebo-controlled trial. Pain Physician. 2013; 16:185–196.
22. Manchikanti L, Rivera JJ, Pampati V, et al. One day lumbar epidural adhesiolysis and hypertonic saline neurolysis in treatment of chronic low back pain: a randomized, double-blind trial. Pain Physician. 2004; 7:177–186.
23. Manchikanti L, Singh V, Cash KA, Pampati V, Datta S. A comparative effectiveness evaluation of percutaneous adhesiolysis and epidural steroid injections in managing lumbar post surgery syndrome: a randomized, equivalence controlled trial. Pain Physician. 2009; 12:E355–E368.
24. Manchikanti L, Cash KA, McManus CD, Pampati V, Singh V, Benyamin R. The preliminary results of a comparative effectiveness evaluation of adhesiolysis and caudal epidural injections in managing chronic low back pain secondary to spinal stenosis: a randomized, equivalence controlled trial. Pain Physician. 2009; 12:E341–E354.
25. Jamison DE, Hsu E, Cohen SP. Epidural adhesiolysis: an evidence-based review. J Neurosurg Sci. 2014; 58:65–76.
 XML Download
XML Download