

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Granular cell tumor is a rare tumor that can originate from the neural system, and it typically occurs in the tongue, breast, skin, and respiratory or digestive tract.1,2,3) Although most granular cell tumors have excellent outcomes after surgical resection, 0.5% to 2% may be malignant and have a poor prognosis with high potential of local recurrence and distant metastasis.3,4) The incidence of granular cell tumors in deep soft tissue of the extremities is very low, especially those of intramuscular origin.2,4,5) In recent researches, there are few reports of intramuscular granular cell tumor. We describe here a case of a granular cell tumor in the sartorius muscle that was successfully treated with surgical resection.
CASE REPORT
A 71-year-old man was referred to Soonchunhyang University Hospital Cheonan with a 10-month history of a non-tender, hard, growing mass in the anterior portion of his right thigh. He had no previous history of any significant underlying illness except for well-controlled hypertension. He had no problems with gait or squatting position. There was no evidence of infection including redness or heating sensation in the right thigh. Laboratory investigations on admission revealed the following: white blood cell count of 5,700, erythrocyte sedimentation rate of 3 mm/h, and C-reactive protein level of 0.3 mg/dl. Abnormal findings were not observed in routine laboratory investigations.
On physical examination, there was an oval-shaped and child-fist sized mass that was located in the anterior aspect of the right thigh. The overlying skin was normal. The mass appeared to be deeply located and arising from the sartorius muscle. The mass was mobile with no tenderness. The patient had no tingling sensation or tinnel sign around mass. A plain radiograph showed normal findings with no osseous abnormality or soft tissue calcification. Ultrasonography showed an ill-defined hypoechoic mass approximately 3.7×3.0 cm in size, which caused acoustic shadowing in the posterior section of the mass (Fig. 1).
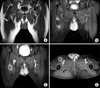
On the preoperative magnetic resonance imaging (MRI), the mass showed a hypointense signal relative to the surrounding muscle, and had an ill-defined margin on T1-weighted sequences. On T2-weighted sequences, the mass had a lower signal intensity than fat, but a slightly higher signal intensity than the muscle. The mass had heterogeneous signal intensity, an ill-defined margin, and a peripheral rim enhancement. There was no bony involvement or abnormal intramedullary signal changes (Fig. 2).
The patient underwent a surgical excision of the tumor. The tumor has more likely benign nature in preoperative MRI, so we performed marginal excision despite of the possibility of malignancy. The mass was carefully dissected from the sartorius muscle using electrocautery. The excised mass was oval-shaped, 6×5×4 cm in size, and had a smooth boundary. On the cut section, the cut surface showed a yellow homogeneous appearance. There was no hemorrhage or necrosis within the tumor. The mass extended to the resection margins of the specimen at multiple points (Fig. 3).
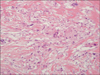
The histological examination revealed that the tumor was composed of ill-defined cords and nests of oval epithelioid cells that had abundant polygonal cells with granular eosinophilic cytoplasm in haematoxylin and eosin stain. There were fibrous septae between the clusters, cells with vesicular nuclei with a prominent nucleolus, eosinophilic granular cytoplasm, and eosinophilic intracytoplasmic particles surrounded by a clear halo (Fig. 4). Histological diagnosis was confirmed with granular cell tumor by two pathologists.
The patient had an ordinary post-operative recovery within two weeks. Partial weight bearing was done with clutch postoperatively. After total stitch out, he was allowed full weight bearing without assistive devices. At the 3-month, 6-month, and 1-year follow-up, the operation site was observed carefully, and there is no evidence of recurrence in physical examination and ultrasonography.
Discussion
The characteristics of granular cell tumor are a solitary painless lesion and unique cytoplasm containing eosinophilic granules.1,6,7) Granular cell tumor usually arises in the nervous system, and can originate in the skin, oral cavity and digestive tract.6,7,8) However, intramuscular granular cell tumor which is located in sartorius muscle is very rare.8) After performing an extensive search of the literature, we could not find any similar cases.
Conventional granular cell tumor is a benign neoplasm. However, malignancy occurs in less than 0.5% to 2% of patients, and they show a higher risk for local recurrence and metastasis with a poor prognosis.3) A large tumor size (>5 cm), older age, female gender, deep location (intramuscular), occurrence in the lower extremities, recent rapid tumor growth after an extended period, and local recurrence are the known factors that increase the malignant potential of granular cell tumor.3,8) The distinction between a benign and malignant granular cell tumor is difficult based on morphology alone, as the different grades are all histologically similar. The diagnosis of malignant granular cell tumor is based on a combination of histological findings, including cellular pleomorphism and elevated mitotic activity, and clinical manifestations.2,8) Because of the possibility of malignancy, wide resection around the tumor is recommended.2,3) Furthermore, Rosenthal et al.9) suggested the application of radiation therapy after complete excision. Although most granular cell tumors are managed successfully with surgical excision, radiation therapy has led to limb preservation and better cosmetic results.9)
In imaging studies, granular cell tumors are best evaluated with MRI. The preoperative MRI is helpful to differentiate this tumor from other soft tissue tumors based on some characteristic findings.4,5,10) Typically, the tumors are slightly hypointense or isointense on T1-weighted sequences, and show homogeneous contrast enhancement after intravenous injection of gadolinium. On T2-weighted sequences, the tumor generally shows heterogeneous increased signal intensity. Peripheral high intensity seems highly specific to granular cell tumors, especially in those of intramuscular origin. This finding corresponds to the lymphocytic infiltration and inflammation noted at the tumor margin.2,10)
In this case, we could successfully treat the patient with complete surgical excision without radiation therapy. The radiation therapy was considered for this patient, but it was not initiated due to old age. After the operation, he had a satisfactory relief of discomfort in his right anterior thigh, and there was no recurrence at 1 year postoperative.
Hence, preoperative MRI should be performed in a patient having clinical manifestations suspicious for intramuscular granular cell tumor. The characteristic MRI findings can help establish the accurate diagnosis and planning resection of the tumor. After establishing the diagnosis, surgeons should remove the tumor completely due to the possibility of malignancy.


 XML Download
XML Download