

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
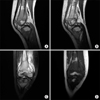
A three-year-old girl presented with a right-sided limp and mild fever. Laboratory findings were normal, except for an elevated erythrocyte sedimentation rate (ESR) of 30 mm/h and a C-reactive protein (CRP) level of 1.5 mg/dl. Magnetic resonance imaging showed a periosteal reaction in the distal posteromedial femur with contour bulging and extension of the reaction to the adjacent vastus muscles. Under a working diagnosis of acute suppurative osteomyelitis, she was initially treated with antibiotics and anti-inflammatory agents for one week. However, this did not result in resolution of her problems or normalization of the ESR and CRP. Biopsies of periosteum and muscle revealed Burkitt lymphoma expressing Bcl-6(+). In a child, limping can be the first clinical sign of hematogenous malignancy. In a limping child, if the general clinical course does not show improvement, and empirical treatment is ineffective, a comprehensive evaluation is necessary, including biopsies or bone marrow aspiration.
Figures and Tables
Figure 1
Widening and irregularity of the epiphyseal plates of the distal femurs, proximal tibias, and distal tibias bilaterally were observed on simple radiographs. A soft tissue shadow indicating a subperiosteal effusion was also observed (arrowheads). In addition, the sclerotic line (arrow) in the metaphysis had to be differentiated from the scurvy lines found in children with vitamin C deficiency.


References
1. Tuten HR, Gabos PG, Kumar SJ, Harter GD. The limping child: a manifestation of acute leukemia. J Pediatr Orthop. 1998; 18:625–629.

2. Widhe B, Widhe T. Initial symptoms and clinical features in osteosarcoma and Ewing sarcoma. J Bone Joint Surg Am. 2000; 82:667–674.
3. Barrios López M, Casado Picón R, de Inocencio Arocena J, Vivanco Martínez JL. Burkitt's lymphoma presenting as an intermittent limp. Reumatol Clin. 2011; 7:139–140.
4. Dierkhuese C, Beattie TF. Acute lymphoblastic leukaemia presenting with atraumatic intermittent limp: a case report. Eur J Emerg Med. 2006; 13:111–112.
5. Sawyer JR, Kapoor M. The limping child: a systematic approach to diagnosis. Am Fam Physician. 2009; 79:215–224.
6. Falcini F, Giani T, Lippi A, Resti M, Simonini G. Recurrent limp in a young boy. Ann Rheum Dis. 2005; 64:500.
7. Houghton KM. Review for the generalist: evaluation of pediatric hip pain. Pediatr Rheumatol Online J. 2009; 7:10.
8. Jang SJ, Yoon DH, Kim S, et al. A unique pattern of extranodal involvement in Korean adults with sporadic Burkitt lymphoma: a single center experience. Ann Hematol. 2012; 91:1917–1922.
9. De Inocencio J. Epidemiology of musculoskeletal pain in primary care. Arch Dis Child. 2004; 89:431–434.
 XML Download
XML Download