

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
An isolated posterior malleolar fracture in the ankle is very rare. We treated eight cases of isolated posterior malleolar fracture, and describe the clinical features and outcomes of treatment.
Materials and Methods
Between from March 2008 to February 2012, eight cases of isolated posterior malleolar fracture were treated in Ilsan Paik Hospital. The mean age of patients was 30 years (11-49 years); six patients were male and five were right. Slip down (4 cases) was the most common injury mechanism. We treated four cases surgically, three cases by cast and one case by ankle brace. We could not recognize three cases of isolated posterior malleolar fracture at first. The time delay to diagnose unrecognized isolated posterior malleolar fracture was nine days, 56 days and 110 days respectively. We were able to diagnose the unrecognized isolated posterior malleolar fracture using computed tomography (two cases) and magnetic resonance imaging (one case).
Results
The main symptom was painful swelling. The average for articular involvement of the posterior malleolar fragment was average 21.4%, and average displacement was 1.25 mm. We treated three cases surgically using a posterior lateral approach and one case using a posterior medial approach. The average American Orthopaedic Foot and Ankle Society score was 92.5 at the last follow-up.
Figures and Tables

Figure 2
Posterior malleolus fragment involves approximately 41% of the distal tibia articular surface on computed tomography scan (Haraguchi type I).
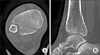
Figure 3
(A, B) Immediate postoperative x-ray showed anatomical reduction of the posterior malleolus. (C, D) After removal of hardware, the x-ray showed a well-united and well-aligned posterior malleolus.

Figure 4
(A, B) Ankle antero-posterior and lateral x-ray showed an undisplaced fracture line at the posterior malleolus. (C, D) Magnetic resonance imaging showed that the minimally displaced isolated posterior malleolar fracture was still not united (Haraguchi type 1).

Figure 5
(A, B) Postoperative radiographs showed anatomical reduction of the posterior mallolar fracture. (C, D) After removal of metal, the fracture was found to be well united.
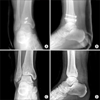
Table 1
Summary of Cases
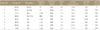
*Initial recognition of fracture. †Number of days diagnosis was delayed. ROM, range of motion; DF, ankle dorsiflexion; PF, ankle plantarflexion; AOFAS, American Orthopaedic Foot and Ankle Society; M, male; F, female; CT, computed tomography; MRI, magnetic resonance imaging; ORIF, open reduction internal fixation.
References
1. Bae SY, Sihn DH. The role of posterior malleolar fragments in ankle pain after trimalleolar fractures. J Korean Soc Fract. 2003; 16:59–66.

2. Harper MC, Hardin G. Posterior malleolar fractures of the ankle associated with external rotation-abduction injuries. Results with and without internal fixation. J Bone Joint Surg Am. 1988; 70:1348–1356.
3. Talbot M, Steenblock TR, Cole PA. Posterolateral approach for open reduction and internal fixation of trimalleolar ankle fractures. Can J Surg. 2005; 48:487–490.
4. Ashhurst APC, Bromer RS. Classification and mechanism of fractures of the leg bones involving the ankle based on a study of three hundred cases from the Episcopal hospital. Arch Surg. 1922; 4:51–129.
5. Quenu E, Mathieu P. Etude critique sur les fractures du cou-de-pied. III. Rev Chir (Paris). 1912; 45:560.
6. Speed K. A discussion of pott's fracture with complications: based on a series of 208 cases. Surg Gynecol Obstet. 1914; 19:73.
7. Haraguchi N, Haruyama H, Toga H, Kato F. Pathoanatomy of posterior malleolar fractures of the ankle. J Bone Joint Surg Am. 2006; 88:1085–1092.
8. Michelson J, Solocoff D, Waldman B, Kendell K, Ahn U. Ankle fractures. The Lauge-Hansen classification revisited. Clin Orthop Relat Res. 1997; 345:198–205.
9. Arimoto HK, Forrester DM. Classification of ankle fractures: an algorithm. AJR Am J Roentgenol. 1980; 135:1057–1063.
10. De Vries JS, Wijgman AJ, Sierevelt IN, Schaap GR. Long-term results of ankle fractures with a posterior malleolar fragment. J Foot Ankle Surg. 2005; 44:211–217.
11. Nugent JF, Gale BD. Isolated posterior malleolar ankle fractures. J Foot Surg. 1990; 29:80–83.
12. Boggs LR. Isolated posterior malleolar fractures. Am J Emerg Med. 1986; 4:334–336.
13. Mingo-Robinet J, López-Durán L, Galeote JE, Martinez-Cervell C. Ankle fractures with posterior malleolar fragment: management and results. J Foot Ankle Surg. 2011; 50:141–145.
14. Neumaier Probst E, Maas R, Meenen NM. Isolated fracture of the posterolateral tibial lip (Volkmann's triangle). Acta Radiol. 1997; 38:359–362.
15. Donken CC, Goorden AJ, Verhofstad MH, Edwards MJ, van Laarhoven CJ. The outcome at 20 years of conservatively treated 'isolated' posterior malleolar fractures of the ankle: a case series. J Bone Joint Surg Br. 2011; 93:1621–1625.
16. Lee JS, Kang SY, Lee HJ, Ko YB. Radiologic analysis and treatment of posterior malleolar fractures of the ankle. J Korean Fract Soc. 2009; 22:98–103.
17. Kim JH, Song JG, Suh JS. The clinical study of ankle fracture and dislocation. J Korean Foot Ankle Soc. 2013; 17:182–188.
 XML Download
XML Download