

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
In order to accurately diagnose lesions of musculoskeletal tissue, evaluation not only of the abnormality of the bone, but the condition of soft tissue is important. Magnetic resonance imaging has been widely used in evaluation of the state of soft tissue, however, it has the disadvantage that testing is expensive and real-time scanning is not possible. In recent years, ultrasonography has been used for evaluation of musculoskeletal tissue and its usefulness has shown a gradual increase. The ultrasound image is determined by the tissue specific acoustic impedance and other factors. Highly reflective tissues such as bone, calcification, ligament, and tendon are expressed as hyperechoic images, and less reflective tissues such as muscle and nerve are expressed as hypoechoic images.
Figures and Tables
Figure 1
Ultrasonography (US) findings of normal skeletal muscle. Long axis (A) and short axis (B) US image of the biceps brachii muscle shows innumerable hyperechoic lines (arrowheads) consistent with perimysium. The epimysium (arrows) demarcates the outer boundaries of the muscle. H, humerus.

Figure 2
Ultrasonography (US) findings of muscle contusion. (A) Long axis US image of the biceps brachii muscle shows a focal hypoechoic defect (arrowheads) within the muscle. (B) Six weeks after injury, resorption of hematoma and regeneration of muscle bundle is observed (arrowheads). B, biceps brachii muscle; H, humerus.

Figure 3
Ultrasonography (US) findings of a normal tendon. (A) Long axis US image of the flexor digitorum tendon (arrows) shows numerous echogenic intratendinous interfaces, resulting in the typical fibrillar appearance. (B) Short axis US image of the flexor digitorum tendon (arrowheads) shows a homogeneous intratendinous pattern made of bright stippled clustered dots.

Figure 4
Long axis ultrasonography image of the supraspinatus tendon shows a focal hypoechoic area (arrowheads) due to anisotrophic artifact. GT, greater tuberosity; SSP, supraspinatus tendon.

Figure 5
Ultrasonography findings of tendinopathy. Long axis image of the extensor carpi radialis brevis tendon shows a focal hypoechoic area (arrows), small calcifications (arrowheads), and loss of fibrillary pattern. LE, lateral epicondyle; RH, radial head.

Figure 6
Ultrasonography (US) findings of rupture of tendon. Long axis (A) and short axis (B) US image of the supraspinatus shows a focal anechoic cleft (arrows). SSP, supraspinatus tendon.

Figure 7
Ultrasonography findings of calcific tendinitis of the shoulder. (A) Type I calcification appears as an intratendinous hyperechoic focus (arrows) with well-defined posterior acoustic shadowing (arrowheads). (B) Type III calcification appears as a hyperechoic focus (arrowheads) with absence of posterior acoustic shadowing.
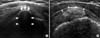
Figure 8
Long axis ultrasonography image of diaphysis of the radius shows a continuous straight hyperechoic line (arrows) and a reverberation artifact (arrowheads) projecting in the shadow beyond the bone can be seen.
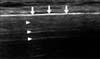
Figure 9
Plain radiographs and ultrasonography (US) findings of mid-clavicle fracture. (A) Plain radiographs of the right clavicle taken six weeks after injury show no callus formation (arrow). (B) US image shows hyperechoic ossified callus formation (arrowheads).

Figure 10
Short axis ultrasonography image of the anterior elbow joint shows a superficial echogenic layer (dashed arrows) related to an acoustical impedance mismatch between cartilage (solid) and adjacent fluid (water), an intermediate hypoechoic band (arrowheads) due to the hyaline cartilage and a deep echogenic layer at the cartilage-subchondral bone interface (arrows).

Figure 11
Long axis ultrasonography image of the posterior shoulder shows a triangular hyperechoic posterior labrum (L). H, humeral head; G, glenoid.
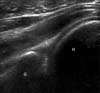
Figure 12
Long axis ultrasonography image over the medial knee shows the normal medial collateral ligament as a thick fibrillar band (arrowheads). F, femur; T, tibia; M, medial meniscus.
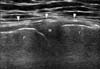
Figure 13
Ultrasonography (US) findings of a normal median nerve. (A) Short axis US image shows well-circumscribed individual structures of different sizes separated by echogenic epineurium (arrowheads). (B) Long axis US image shows the nerve fascicles appearing as elongated hypoechoic bands (arrowheads) that run parallel to each other. The internal epineurium (arrows) separates them more clearly. M, median nerve; T, flexor tendon.

References
1. Moosmayer S, Smith HJ. Diagnostic ultrasound of the shoulder--a method for experts only? Results from an orthopedic surgeon with relative inexpensive compared to operative findings. Acta Orthop. 2005; 76:503–508.
2. Lehto M, Alanen A. Healing of a muscle trauma. Correlation of sonographical and histological findings in an experimental study in rats. J Ultrasound Med. 1987; 6:425–429.

3. Campbell RS, Grainger AJ. Current concepts in imaging of tendinopathy. Clin Radiol. 2001; 56:253–267.
4. Khan KM, Bonar F, Desmond PM, et al. Victorian Institute of Sport Tendon Study Group. Patellar tendinosis (jumper's knee): findings at histopathologic examination, US, and MR imaging. Radiology. 1996; 200:821–827.
5. Fornage BD, Rifkin MD, Touche DH, Segal PM. Sonography of the patellar tendon: preliminary observations. AJR Am J Roentgenol. 1984; 143:179–182.
6. Maffulli N, Regine R, Carrillo F, Capasso G, Minelli S. Tennis elbow: an ultrasonographic study in tennis players. Br J Sports Med. 1990; 24:151–155.
7. Martinoli C, Derchi LE, Pastorino C, Bertolotto M, Silvestri E. Analysis of echotexture of tendons with US. Radiology. 1993; 186:839–843.
8. Farin PU, Jaroma H, Harju A, Soimakallio S. Medial displacement of the biceps brachii tendon: evaluation with dynamic sonography during maximal external shoulder rotation. Radiology. 1995; 195:845–848.
9. Fessell DP, Vanderschueren GM, Jacobson JA, et al. US of the ankle: technique, anatomy, and diagnosis of pathologic conditions. Radiographics. 1998; 18:325–340.
10. Prato N, Abello E, Martinoli C, Derchi L, Bianchi S. Sonography of posterior tibialis tendon dislocation. J Ultrasound Med. 2004; 23:701–705.
11. Barata I, Spencer R, Suppiah A, Raio C, Ward MF, Sama A. Emergency ultrasound in the detection of pediatric long-bone fractures. Pediatr Emerg Care. 2012; 28:1154–1157.
12. Rabiner JE, Friedman LM, Khine H, Avner JR, Tsung JW. Accuracy of point-of-care ultrasound for diagnosis of skull fractures in children. Pediatrics. 2013; 131:e1757–e1764.
13. Rabiner JE, Khine H, Avner JR, Friedman LM, Tsung JW. Accuracy of point-of-care ultrasonography for diagnosis of elbow fractures in children. Ann Emerg Med. 2013; 61:9–17.
14. Matsuyama J, Ohnishi I, Sakai R, et al. A new method for evaluation of fracture healing by echo tracking. Ultrasound Med Biol. 2008; 34:775–783.
15. Weiss DB, Jacobson JA, Karunakar MA. The use of ultrasound in evaluating orthopaedic trauma patients. J Am Acad Orthop Surg. 2005; 13:525–533.
16. Smith J, Dahm DL, Newcomer-Aney KL. Role of sonography in the evaluation of unstable os acromiale. J Ultrasound Med. 2008; 27:1521–1526.
17. Peetrons P, Creteur V, Bacq C. Sonography of ankle ligaments. J Clin Ultrasound. 2004; 32:491–499.
18. Brasseur JL, Morvan G, Godoc B. Dynamic ultrasonography. J Radiol. 2005; 86:1904–1910.
19. Buchberger W, Schön G, Strasser K, Jungwirth W. High-resolution ultrasonography of the carpal tunnel. J Ultrasound Med. 1991; 10:531–537.
 XML Download
XML Download