

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
Subaxial unilateral facet dislocation requires immediate reduction; however, cases of failure with reduction have also been reported. We analyzed the factors preventing closed traction reduction and attempted to determine the efficacy and indications of closed traction reduction.
Materials and Methods
We selected 26 patients, 17 men and nine women. The average age of the patients in selected group was 49 years (20-69 years). Each patient was first treated with Gardner head traction and closed traction reduction. Each patient was checked for the degree of locking of the dislocated segment, intervertebral disc herniation, the degree of contralateral facet joint subluxation, and accompanied fracture. The effect of the location of the injured segment, age, and sex on closed reduction traction was analyzed.
Results
A high rate of unsuccessful closed traction reduction was observed for patients with more than 50% locking of the dislocated facet joint (p=0.039). Intervertebral disc herniation, the degree of contralateral facet joint subluxation, facet joint fracture, and pedicle and lamina fracture were unrelated to the success of closed traction reduction. The location of dislocation and sex showed no statistically significant relevance to failure of closed traction reduction. A high rate of failure was observed for patients younger than 40 years. Of the 26 patients, closed traction reduction was successful for 12 and unsuccessful for 14.
Conclusion
For patients whose degree of locking of the dislocated facet joint is less than 50%, closed traction reduction using skull traction is considered effective, however, for patients younger than 40 years or with more than 50% locking of the dislocated facet, prompt reduction under general anesthesia and subsequent appropriate surgery is considered beneficial.
Figures and Tables
Figure 1
(A) This radiograph shows a unilateral facet dislocation in a 30-year-old male at C3-4 level, (B) shows that closed reduction failed by Gardner-Well tongs traction. (C) T2 sagittal magnetic resonance imaging; (D) Left side sagittal computed tomography (CT) image; (E) Right side sagittal CT image. (F) This radiograph shows spontaneous reduction of a dislocated facet at C3-4 level without manipulation after anesthesia.
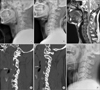
Figure 2
(A) Lateral view radiograph of a 31-year-old male. Listhesis of C6 on C7 with dislocation of the left unilateral facet joint. Unilateral complete interlocking of the articular facets is shown. (B) Lateral view radiograph of a 61-year-old male. Listhesis of C5 on C6 with dislocation of the right unilateral facet joint.


References
1. Stauffer ES. Fractures and dislocations of the spine: part 1. The cervical spine. In : Rockwood CA, Green DP, editors. Fractures in adults. 2nd ed. Philadelphia: Lippincott;1984.
2. Stauffer ES, Kelly EG. Fracture-dislocations of the cervical spine. Instability and recurrent deformity following treatment by anterior interbody fusion. J Bone Joint Surg Am. 1977; 59:45–48.

3. Van Peteghem PK, Schweigel JF. The fractured cervical spine rendered unstable by anterior cervical fusion. J Trauma. 1979; 19:110–114.
4. Star AM, Jones AA, Cotler JM, Balderston RA, Sinha R. Immediate closed reduction of cervical spine dislocations using traction. Spine (Phila Pa 1976). 1990; 15:1068–1072.
5. Vital JM, Gille O, Sénégas J, Pointillart V. Reduction technique for uni- and biarticular dislocations of the lower cervical spine. Spine (Phila Pa 1976). 1998; 23:949–954.
6. O'Brien PJ, Schweigel JF, Thompson WJ. Dislocations of the lower cervical spine. J Trauma. 1982; 22:710–714.
7. Grant GA, Mirza SK, Chapman JR, et al. Risk of early closed reduction in cervical spine subluxation injuries. J Neurosurg. 1999; 90:1 Suppl. 13–18.
8. Rizzolo SJ, Vaccaro AR, Cotler JM. Cervical spine trauma. Spine (Phila Pa 1976). 1994; 19:2288–2298.
9. Lowery DW, Wald MM, Browne BJ, Tigges S, Hoffman JR, Mower WR. NEXUS Group. Epidemiology of cervical spine injury victims. Ann Emerg Med. 2001; 38:12–16.
10. Andreshak JL, Dekutoski MB. Management of unilateral facet dislocations: a review of the literature. Orthopedics. 1997; 20:917–926.
11. Levine AM, Mazel C, Roy-Camille R. Management of fracture separations of the articular mass using posterior cervical plating. Spine (Phila Pa 1976). 1992; 17:S447–S454.
12. Crawford NR, Duggal N, Chamberlain RH, Park SC, Sonntag VK, Dickman CA. Unilateral cervical facet dislocation: injury mechanism and biomechanical consequences. Spine (Phila Pa 1976). 2002; 27:1858–1864.
13. Cotler JM, Herbison GJ, Nasuti JF, Ditunno JF Jr, An H, Wolff BE. Closed reduction of traumatic cervical spine dislocation using traction weights up to 140 pounds. Spine (Phila Pa 1976). 1993; 18:386–390.
14. Robertson PA, Ryan MD. Neurological deterioration after reduction of cervical subluxation. Mechanical compression by disc tissue. J Bone Joint Surg Br. 1992; 74:224–227.
15. Lee AS, MacLean JC, Newton DA. Rapid traction for reduction of cervical spine dislocations. J Bone Joint Surg Br. 1994; 76:352–356.
16. Mahale YJ, Silver JR, Henderson NJ. Neurological complications of the reduction of cervical spine dislocations. J Bone Joint Surg Br. 1993; 75:403–409.
17. Olerud C, Jónsson H Jr. Compression of the cervical spine cord after reduction of fracture dislocations. Report of 2 cases. Acta Orthop Scand. 1991; 62:599–601.
18. Vaccaro AR, Falatyn SP, Flanders AE, Balderston RA, Northrup BE, Cotler JM. Magnetic resonance evaluation of the intervertebral disc, spinal ligaments, and spinal cord before and after closed traction reduction of cervical spine dislocations. Spine (Phila Pa 1976). 1999; 24:1210–1217.
19. Tribus CB. Cervical disk herniation in association with traumatic facet dislocation. Tech Orthop. 1994; 9:5–7.
20. Fried LC. Cervical spinal cord injury during skeletal traction. JAMA. 1974; 229:181–183.
21. Bohlman HH, Ducker TB, Lacas JT. Spine and spinal cord injuries. In : Rothman RH, Simeone FA, editors. The spine. Philadelphia: Saunders;1982. p. 661–757.
22. White AA, Southwick WO, Panjabi MM. Clinical instability in the lower cervical spine: a review of past and current concepts. Spine (Phila Pa 1976). 1976; 1:15–27.
23. Sabiston CP, Wing PC, Schweigel JF, Van Peteghem PK, Yu W. Closed reduction of dislocations of the lower cervical spine. J Trauma. 1988; 28:832–835.
24. Andreshak JL, Dekutoski MB. Management of unilateral facet dislocations: a review of the literature. Orthopedics. 1997; 20:917–926.
25. Rorabeck CH, Rock MG, Hawkins RJ, Bourne RB. Unilateral facet dislocation of the cervical spine. An analysis of the results of treatment in 26 patients. Spine (Phila Pa 1976). 1987; 12:23–27.
 XML Download
XML Download